Gao Amy, Osgood Nathaniel D, Jiang Ying, Dyck Roland F
Strategic Planning and Data Warehousing, University of Alberta, Edmonton, Canada.
Department of Computer Science, University of Saskatchewan, Saskatoon, Canada.
BMC Nephrol. 2017 Sep 4;18(1):283. doi: 10.1186/s12882-017-0699-y.
Diabetes-related end stage renal disease (DM-ESRD) is a devastating consequence of the type 2 diabetes epidemic, both of which disproportionately affect Indigenous peoples. Projecting case numbers and costs into future decades would help to predict resource requirements, and simulating hypothetical interventions could guide the choice of best practices to mitigate current trends.
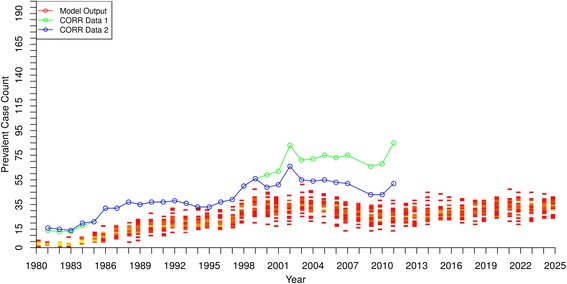
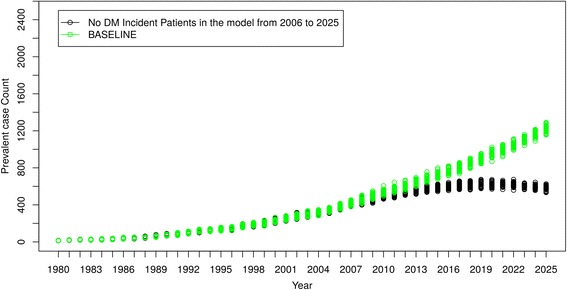
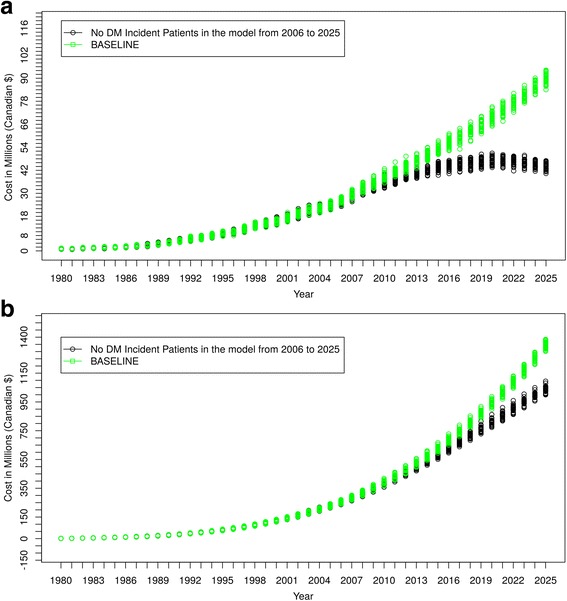
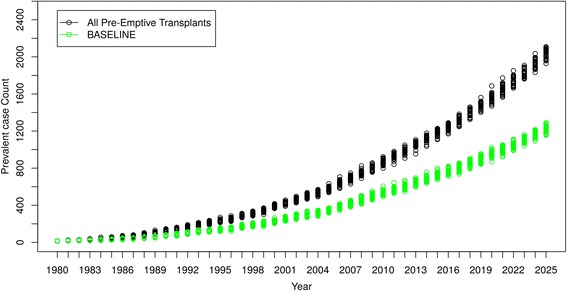
An agent based model (ABM) was built to forecast First Nations and non-First Nations cases of DM-ESRD in Saskatchewan from 1980 to 2025 and to simulate two hypothetical interventions. The model was parameterized with data from the Canadian Institute for Health Information, Saskatchewan Health Administrative Databases, the Canadian Organ Replacement Register, published studies and expert judgement. Input parameters without data sources were estimated through model calibration. The model incorporated key patient characteristics, stages of diabetes and chronic kidney disease, renal replacement therapies, the kidney transplant assessment and waiting list processes, costs associated with treatment options, and death. We used this model to simulate two interventions: 1) No new cases of diabetes after 2005 and 2) Pre-emptive renal transplants carried out on all diabetic persons with new ESRD.
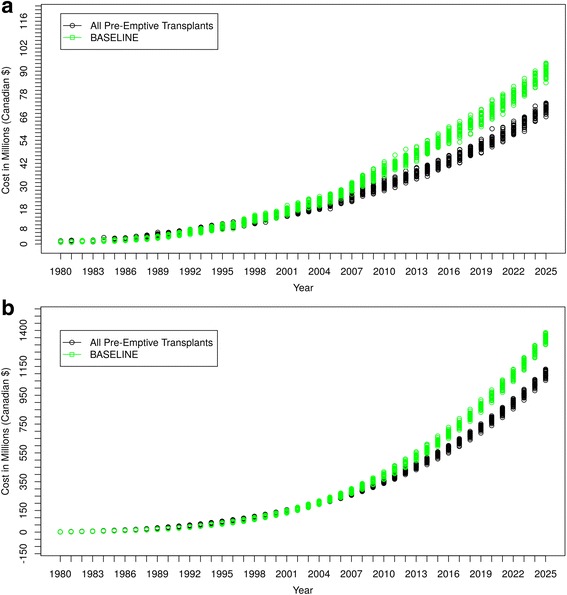
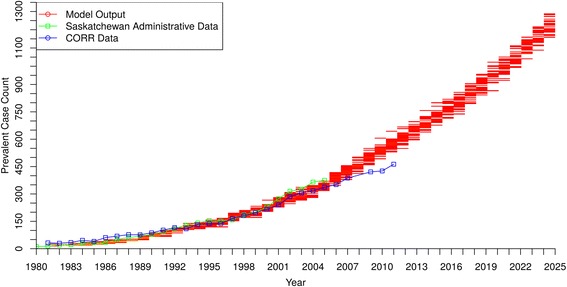
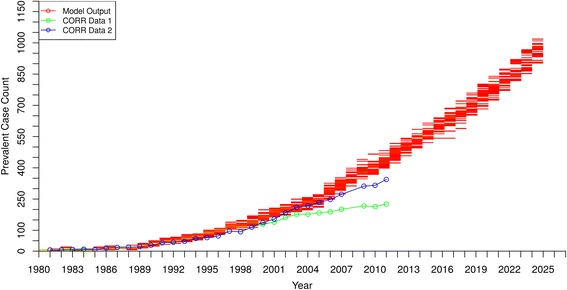
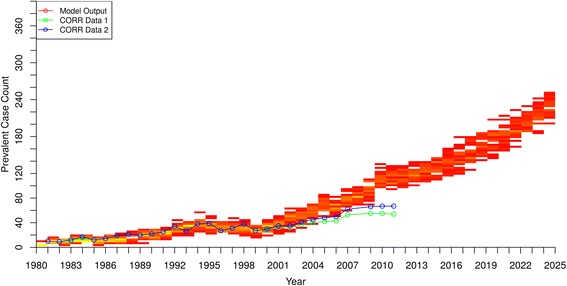
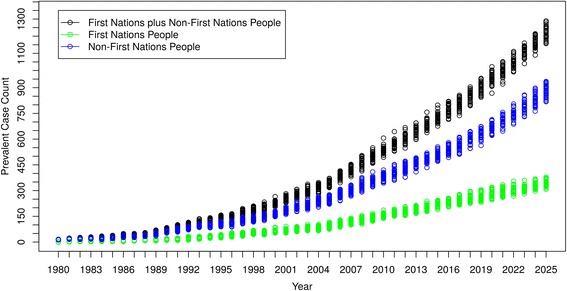
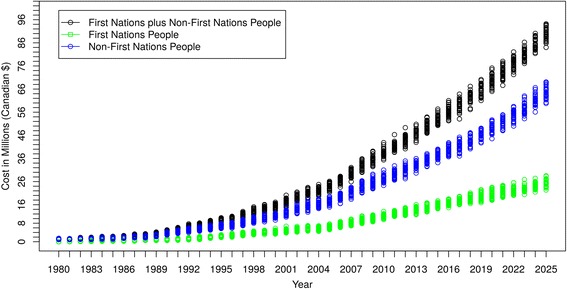
There was a close match between empirical data and model output. Going forward, both incidence and prevalence cases of DM-ESRD approximately doubled from 2010 to 2025, with 250-300 new cases per year and almost 1300 people requiring RRT by 2025. Prevalent cases of First Nations people with DM-ESRD increased from 19% to 27% of total DM-ESRD numbers from 1990 to 2025. The trend in yearly costs paralleled the prevalent DM-ESRD case count. For Scenario 1, despite eliminating diabetes incident cases after 2005, prevalent cases of DM-ESRD continued to rise until 2019 before slowly declining. When all DM-ESRD incident cases received a pre-emptive renal transplant (scenario 2), a substantial increase in DM-ESRD prevalence occurred reflecting higher survival, but total costs decreased reflecting the economic advantage of renal transplantation.
This ABM can forecast numbers and costs of DM-ESRD in Saskatchewan and be modified for application in other jurisdictions. This can aid in resource planning and be used by policy makers to evaluate different interventions in a safe and economical manner.
糖尿病相关终末期肾病(DM-ESRD)是2型糖尿病流行带来的灾难性后果,这两者对原住民的影响尤为严重。预测未来几十年的病例数和成本将有助于预测资源需求,模拟假设干预措施可以指导选择最佳实践以缓解当前趋势。
构建了一个基于主体的模型(ABM),以预测1980年至2025年萨斯喀彻温省原住民和非原住民的DM-ESRD病例,并模拟两种假设干预措施。该模型使用了来自加拿大卫生信息研究所、萨斯喀彻温省卫生行政数据库、加拿大器官替代登记处、已发表研究和专家判断的数据进行参数化。没有数据源的输入参数通过模型校准进行估计。该模型纳入了关键患者特征、糖尿病和慢性肾病阶段、肾脏替代疗法、肾脏移植评估和等待名单流程、与治疗选择相关的成本以及死亡情况。我们使用该模型模拟了两种干预措施:1)2005年后无新增糖尿病病例;2)对所有新患ESRD的糖尿病患者进行抢先肾移植。
实证数据与模型输出结果高度匹配。展望未来,2010年至2025年期间,DM-ESRD的发病率和患病率几乎翻了一番,每年有250 - 300例新病例,到2025年近1300人需要肾脏替代治疗。1990年至2025年期间,患有DM-ESRD的原住民病例在DM-ESRD总数中的占比从19%增至27%。年度成本趋势与DM-ESRD现患病例数平行。对于情景1,尽管2005年后消除了糖尿病新发病例,但DM-ESRD现患病例数持续上升至2019年,之后缓慢下降。当所有DM-ESRD新发病例接受抢先肾移植时(情景2),DM-ESRD患病率大幅上升,反映出更高的生存率,但总成本下降,反映出肾移植的经济优势。
该ABM可以预测萨斯喀彻温省DM-ESRD的病例数和成本,并可进行修改以应用于其他司法管辖区。这有助于资源规划,并可供政策制定者以安全且经济的方式评估不同的干预措施。