Singal Ashwani K, Jackson Bradford, Pereira Glauber B, Russ Kirk B, Fitzmorris Paul Stephen, Kakati Donny, Axley Page, Ravi Sujan, Seay Toni, Ramachandra Rao Satish P, Mehta Ravindra, Kuo Yong-Fang, Singh Karan P, Agarwal Anupam
Division of Gastroenterology and Hepatology, Department of Medicine, University of Alabama, Birmingham, AL, USA.
Nephron. 2018;138(1):1-12. doi: 10.1159/000479074. Epub 2017 Sep 2.
To define urine or serum biomarkers in predicting renal function recovery after liver transplantation (LT).
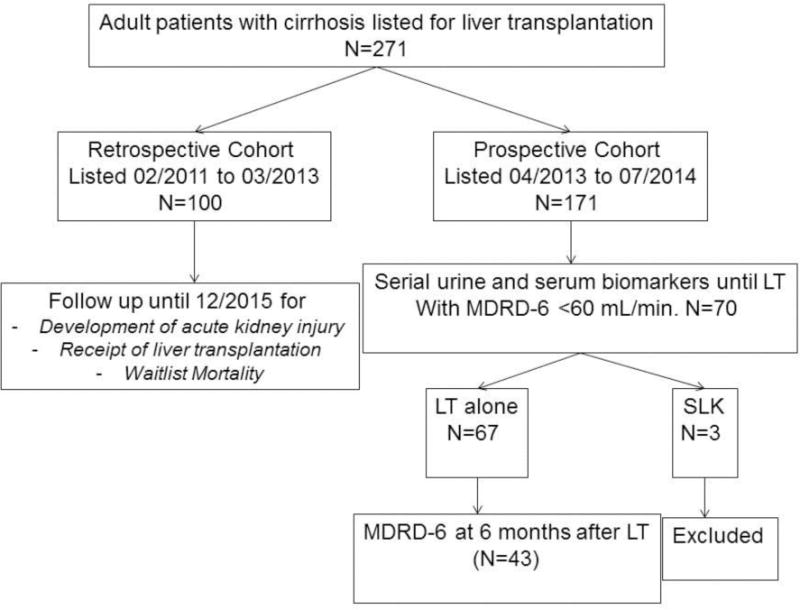
Adults listed for LT (February 2011-July 2014) and with modified diet for renal disease-6 (MDRD-6) <60 mL/min provided urine/blood samples at baseline and serially until LT for biomarkers in serum (pg/mL) and urine (pg/mg creatinine).
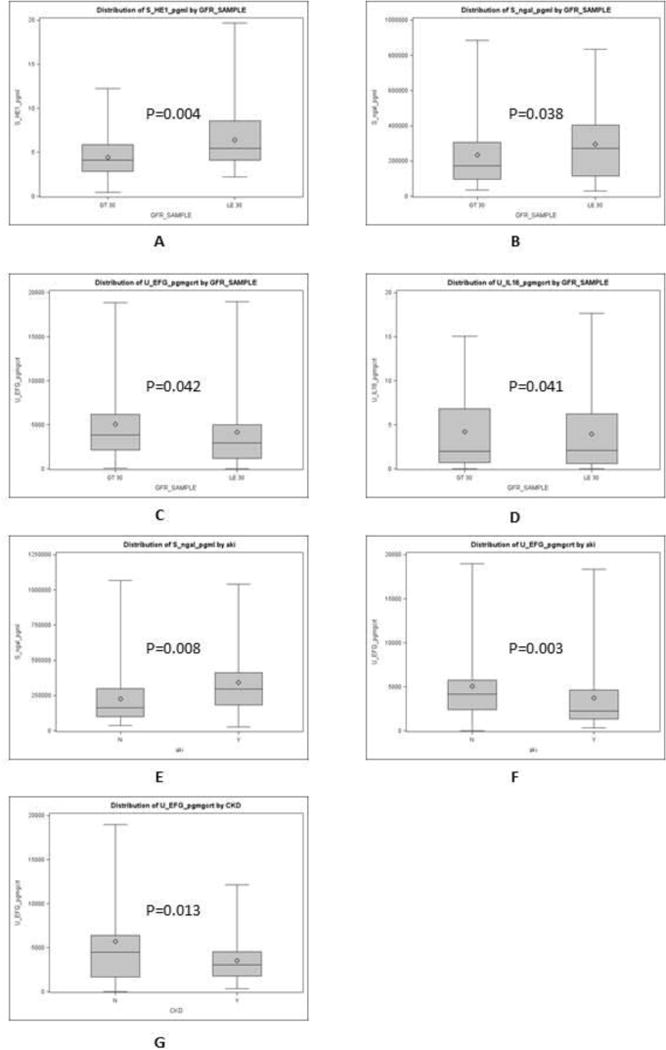
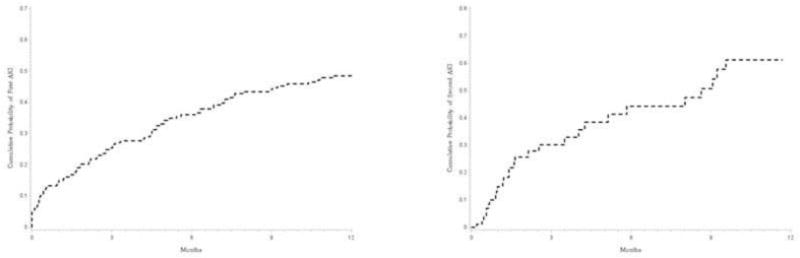
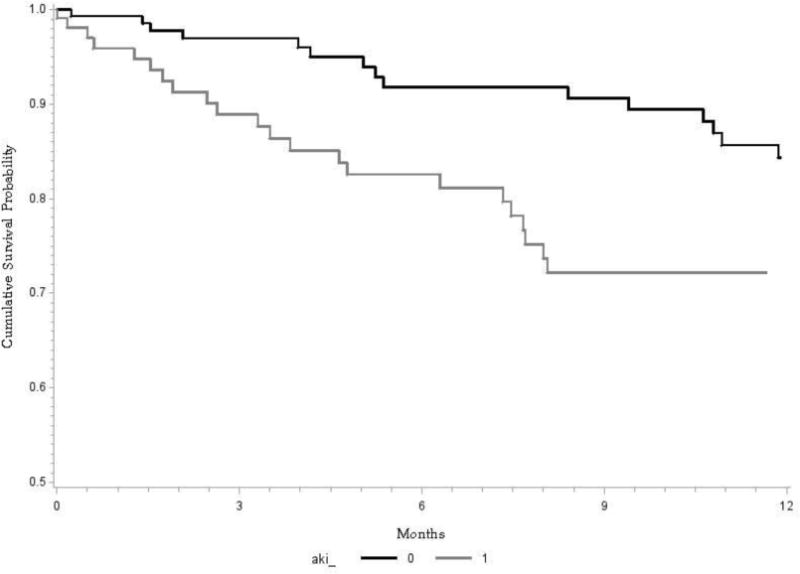
Of 271 LT listed patients (mean age 57 years, 63% males, median listing MELD 17.5), 1 year acute kidney injury (AKI) probability was 49%, with odds of 1.3-, 3.0-, 4.6-, and 8.5-fold times for listing MELD 16-20, 21-25, 26-30, and >30, compared to MELD <16. Thirty-seven people died over 1 year from the time of listing, with twofold increased odds with AKI. Among 67 patients with MDRD <60, only urinary epidermal growth factor was different comparing AKI (increase in serum creatinine ≥0.3 mg/dL from baseline within past 3 months) vs. no AKI (2,254 vs. 4,253, p = 0.003). Differences between acute tubular necrosis (ATN) and hepatorenal syndrome could not be ascertained for a small sample of 3 patients with ATN. Analyzing 15 of 43 receiving LT and MDRD-6 <30 prior to LT, biomarkers were not different comparing 5 patients recovering renal function (MDRD-6 >50 mL/min) at 6 months vs. 10 without recovery.
AKI is common among LT listed patients, with a negative impact on transplant-free survival. Serum and urine biomarkers are not associated with the recovery of renal function after LT. Multicenter studies are suggested to (a) develop strategies to reduce the development of AKI and (b) derive novel biomarkers for use in accurately predicting renal recovery after LT.
确定尿液或血清生物标志物以预测肝移植(LT)后肾功能的恢复情况。
2011年2月至2014年7月被列入LT名单且改良肾病饮食-6(MDRD-6)<60 mL/min的成年人在基线时提供尿液/血液样本,并持续采样直至LT,用于检测血清(pg/mL)和尿液(pg/mg肌酐)中的生物标志物。
在271名被列入LT名单的患者中(平均年龄57岁,63%为男性,列入名单时的中位终末期肝病模型评分(MELD)为17.5),1年急性肾损伤(AKI)的概率为49%,与MELD<16相比,列入名单时MELD为16-20、21-25、26-30和>30的患者发生AKI的几率分别为1.3倍、3.0倍、4.6倍和8.5倍。从列入名单开始的1年中有37人死亡,AKI患者的死亡几率增加了一倍。在67名MDRD<60的患者中,仅尿表皮生长因子在AKI(过去3个月内血清肌酐较基线升高≥0.3 mg/dL)与无AKI患者之间存在差异(2254对4253,p = 0.003)。对于3例急性肾小管坏死(ATN)患者的小样本,无法确定ATN与肝肾综合征之间的差异。分析43例LT前MDRD-6<30的患者中的15例,6个月时肾功能恢复(MDRD-6>50 mL/min)的5例患者与10例未恢复的患者相比,生物标志物无差异。
AKI在被列入LT名单的患者中很常见,对无移植生存期有负面影响。血清和尿液生物标志物与LT后肾功能的恢复无关。建议开展多中心研究以(a)制定减少AKI发生的策略,以及(b)获得用于准确预测LT后肾功能恢复的新型生物标志物。