Jowett Sue, Barton Pelham, Roalfe Andrea, Fletcher Kate, Hobbs F D Richard, McManus Richard J, Mant Jonathan
Health Economics Unit, Institute of Applied Health Research, University of Birmingham, West Midlands, United Kingdom.
Primary Care Clinical Sciences, Institute of Applied Health Research, University of Birmingham, West Midlands, United Kingdom.
PLoS One. 2017 Sep 5;12(9):e0182625. doi: 10.1371/journal.pone.0182625. eCollection 2017.
Clinical trials suggest that use of fixed-dose combination therapy ('polypills') can improve adherence to medication and control of risk factors of people at high risk of cardiovascular disease (CVD) compared to usual care, but cost-effectiveness is unknown.
To determine whether a polypill is cost-effective compared to usual care and optimal guideline-recommended treatment for primary prevention in people already on statins and/or blood pressure lowering therapy.
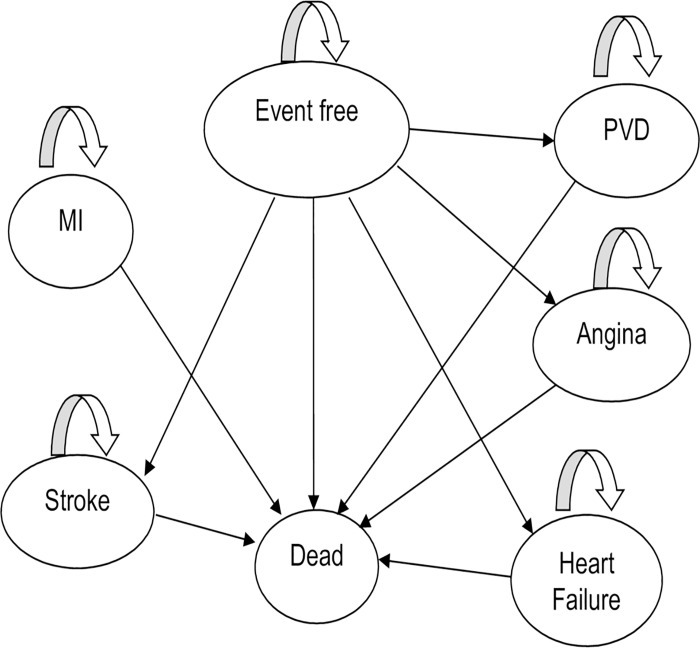
A Markov model was developed to perform a cost-utility analysis with a one year time cycle and a 10 year time horizon to compare the polypill with usual care and optimal implementation of NICE Guidelines, using patient level data from a retrospective cross-sectional study. The model was run for ten age (40 years+) and gender-specific sub-groups on treatment for raised CVD risk with no history of CVD. Published sources were used to estimate impact of different treatment strategies on risk of CVD events.
A polypill strategy was potentially cost-effective compared to other strategies for most sub-groups ranging from dominance to up to £18,811 per QALY depending on patient sub-group. Optimal implementation of guidelines was most cost-effective for women aged 40-49 and men aged 75+. Results were sensitive to polypill cost, and if the annual cost was less than £150, this approach was cost-effective compared to the other strategies.
For most people already on treatment to modify CVD risk, a polypill strategy may be cost-effective compared with optimising treatment as per guidelines or their current care, as long as the polypill cost is sufficiently low.
临床试验表明,与常规治疗相比,使用固定剂量联合疗法(“复方药丸”)可提高心血管疾病(CVD)高危人群的用药依从性并控制危险因素,但成本效益尚不清楚。
确定与常规治疗以及针对已接受他汀类药物和/或降压治疗的人群进行一级预防的最佳指南推荐治疗相比,复方药丸是否具有成本效益。
开发了一个马尔可夫模型,以一年为时间周期、十年为时间跨度进行成本效用分析,使用一项回顾性横断面研究中的患者层面数据,将复方药丸与常规治疗以及英国国家卫生与临床优化研究所(NICE)指南的最佳实施情况进行比较。该模型针对十个年龄(40岁及以上)和按性别划分的亚组进行运行,这些亚组正在接受治疗以降低CVD风险且无CVD病史。使用已发表的资料来估计不同治疗策略对CVD事件风险的影响。
对于大多数亚组而言,与其他策略相比,复方药丸策略可能具有成本效益,从优势到每质量调整生命年高达18,811英镑不等,具体取决于患者亚组。指南的最佳实施对于40 - 49岁的女性和75岁及以上的男性最具成本效益。结果对复方药丸成本敏感,如果年度成本低于150英镑,与其他策略相比,这种方法具有成本效益。
对于大多数已经在接受治疗以改变CVD风险的人来说,只要复方药丸成本足够低,与按照指南优化治疗或其当前治疗相比,复方药丸策略可能具有成本效益。