School of Public Health, Sun Yat-sen University, Guangzhou, 510080, Guangdong, People's Republic of China.
MRC Integrative Epidemiology Unit, University of Bristol, Rm OS11, Oakfield House, Oakfield Grove, Bristol, BS8 2BN, UK.
Diabetologia. 2017 Nov;60(11):2210-2220. doi: 10.1007/s00125-017-4396-y. Epub 2017 Sep 9.
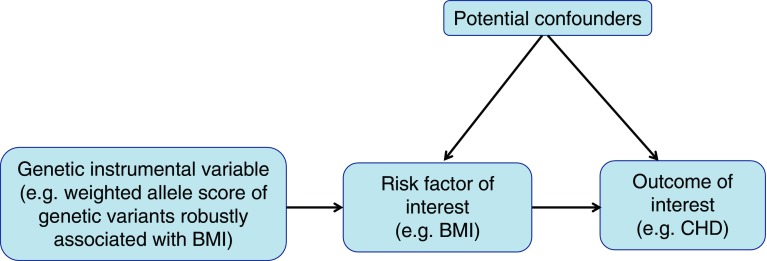
AIMS/HYPOTHESIS: The extent to which effects of BMI on CHD are mediated by glycaemic and lipid risk factors is unclear. In this study we examined the effects of these traits using genetic evidence.
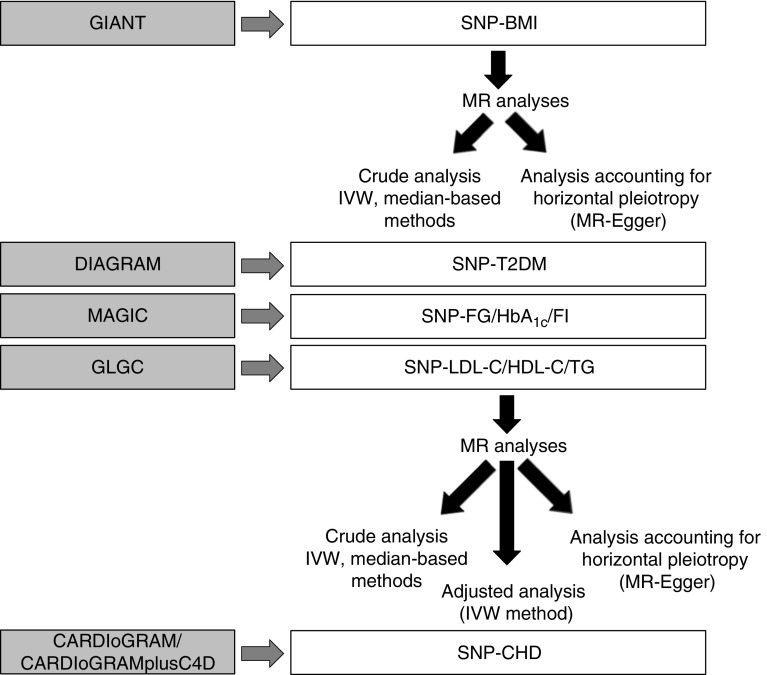
We used two-sample Mendelian randomisation to determine: (1) the causal effect of BMI on CHD (60,801 case vs 123,504 control participants), type 2 diabetes (34,840 case vs 114,981 control participants), fasting glucose (n = 46,186), insulin (n = 38,238), HbA (n = 46,368) and LDL-cholesterol, HDL-cholesterol and triacylglycerols (n = 188,577); (2) the causal effects of glycaemic and lipids traits on CHD; and (3) the extent to which these traits mediate any effect of BMI on CHD.
One SD higher BMI (~ 4.5 kg/m) was associated with higher risk of CHD (OR 1.45 [95% CI 1.27, 1.66]) and type 2 diabetes (1.96 [95% CI 1.35, 2.83]), higher levels of fasting glucose (0.07 mmol/l [95% CI 0.03, 0.11]), HbA (0.05% [95% CI 0.01, 0.08]), fasting insulin (0.18 log pmol/l [95% CI 0.14, 0.22]) and triacylglycerols (0.20 SD [95% CI 0.14, 0.26]) and lower levels of HDL-cholesterol (-0.23 SD [95% CI -0.32, -0.15]). There was no evidence for a causal relation between BMI and LDL-cholesterol. The causal associations of higher triacylglycerols, HbA and diabetes risk with CHD risk remained after performing sensitivity analyses that considered different models of horizontal pleiotropy. The BMI-CHD effect reduced from 1.45 to 1.16 (95% CI 0.99, 1.36) and to 1.36 (95% CI 1.19, 1.57) with genetic adjustment for triacylglycerols or HbA, respectively, and to 1.09 (95% CI 0.94, 1.27) with adjustment for both.
CONCLUSIONS/INTERPRETATION: Increased triacylglycerol levels and poor glycaemic control appear to mediate much of the effect of BMI on CHD.
目的/假设:BMI 对 CHD 的影响在多大程度上受到血糖和血脂风险因素的影响尚不清楚。在这项研究中,我们使用遗传证据来研究这些特征的影响。
我们使用两样本 Mendelian 随机化来确定:(1)BMI 对 CHD(60801 例病例与 123504 例对照参与者)、2 型糖尿病(34840 例病例与 114981 例对照参与者)、空腹血糖(n=46186)、胰岛素(n=38238)、糖化血红蛋白(n=46368)和 LDL-胆固醇、HDL-胆固醇和三酰甘油(n=188577)的因果效应;(2)血糖和脂质特征对 CHD 的因果效应;(3)这些特征在多大程度上介导了 BMI 对 CHD 的影响。
SD 更高的 BMI(~4.5kg/m)与 CHD(OR 1.45[95%CI 1.27, 1.66])和 2 型糖尿病(1.96[95%CI 1.35, 2.83])的风险增加、空腹血糖(0.07mmol/l[95%CI 0.03, 0.11])、糖化血红蛋白(0.05%[95%CI 0.01, 0.08])、空腹胰岛素(0.18log pmol/l[95%CI 0.14, 0.22])和三酰甘油(0.20SD[95%CI 0.14, 0.26])水平升高以及 HDL-胆固醇(-0.23SD[95%CI -0.32, -0.15])水平降低有关。BMI 与 LDL-胆固醇之间没有因果关系的证据。在进行考虑水平遗传异质性的不同模型的敏感性分析后,较高的三酰甘油、HbA 和糖尿病风险与 CHD 风险之间的因果关系仍然存在。当用三酰甘油或糖化血红蛋白进行遗传调整时,BMI-CHD 效应从 1.45 分别降至 1.16(95%CI 0.99, 1.36)和 1.36(95%CI 1.19, 1.57),当同时调整两者时,BMI-CHD 效应降至 1.09(95%CI 0.94, 1.27)。
结论/解释:甘油三酯水平升高和血糖控制不佳似乎介导了 BMI 对 CHD 的大部分影响。