Ren Song, Wang Ying, Xian Li, Toyama Tadashi, Jardine Meg, Li Guisen, Perkovic Vlado, Hong Daqing
Renal Division and Institute of Nephrology, Sichuan Academy of Medical Science & Sichuan Provincial People's Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, China.
The George Institute for Global Health, University of Sydney, Sydney, Australia.
PLoS One. 2017 Sep 12;12(9):e0184398. doi: 10.1371/journal.pone.0184398. eCollection 2017.
Immunosuppressive agents in general are shown to prevent renal progression and all-cause mortality in idiopathic membranous nephropathy (IMN) patients with nephrotic syndrome. However, the efficacy and safety of different immunosuppressive treatments have not been systematic assessed and compared. A network meta-analysis was performed to compare different immunosuppressive treatment in IMN.
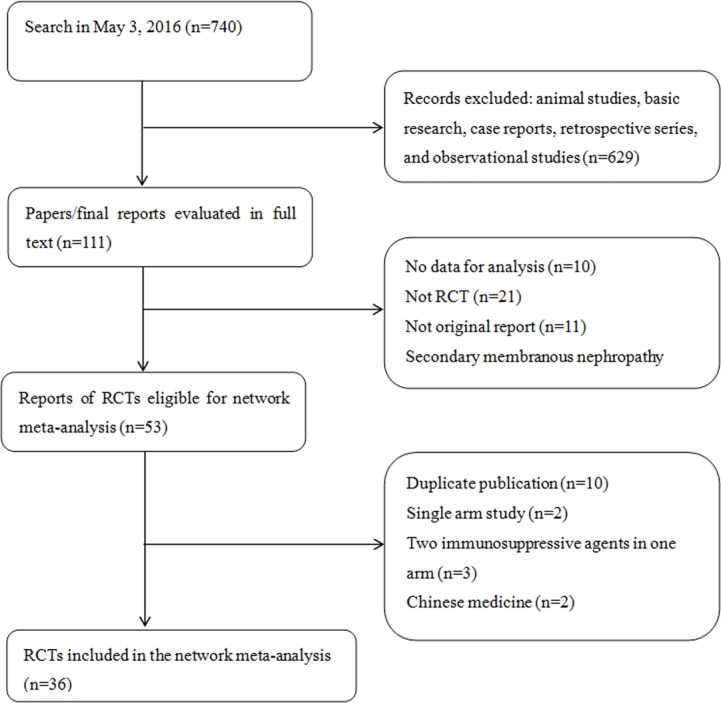
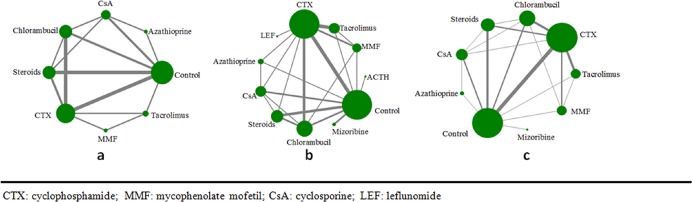
Cochrane library, MEDLINE, EMBASE and trial register system were searched for randomized controlled trials reporting the treatments for IMN to May 3, 2016. Composite endpoint of mortality or end-stage kidney disease (ESKD), complete or partial proteinuria remission and withdrawal because of treatment adverse events were compared combing direct and indirect comparison using network meta-analysis. Ranking different immunosuppressive treatments in the outcomes were analyzed by using surface under the cumulative ranking curve (SUCRA).
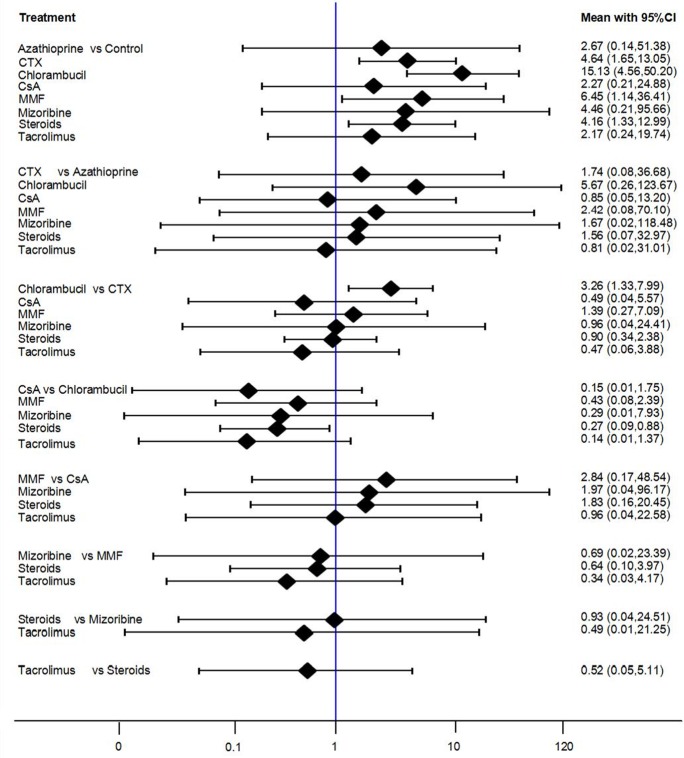
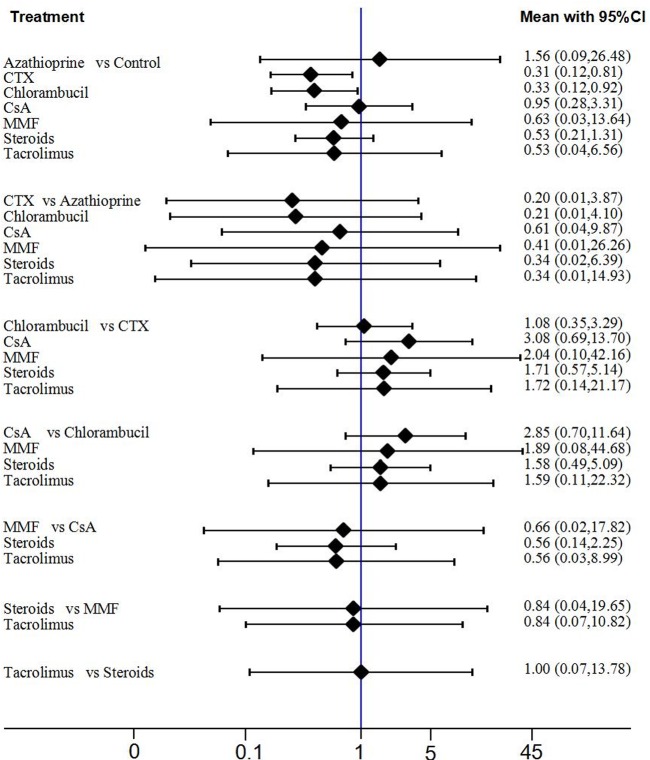
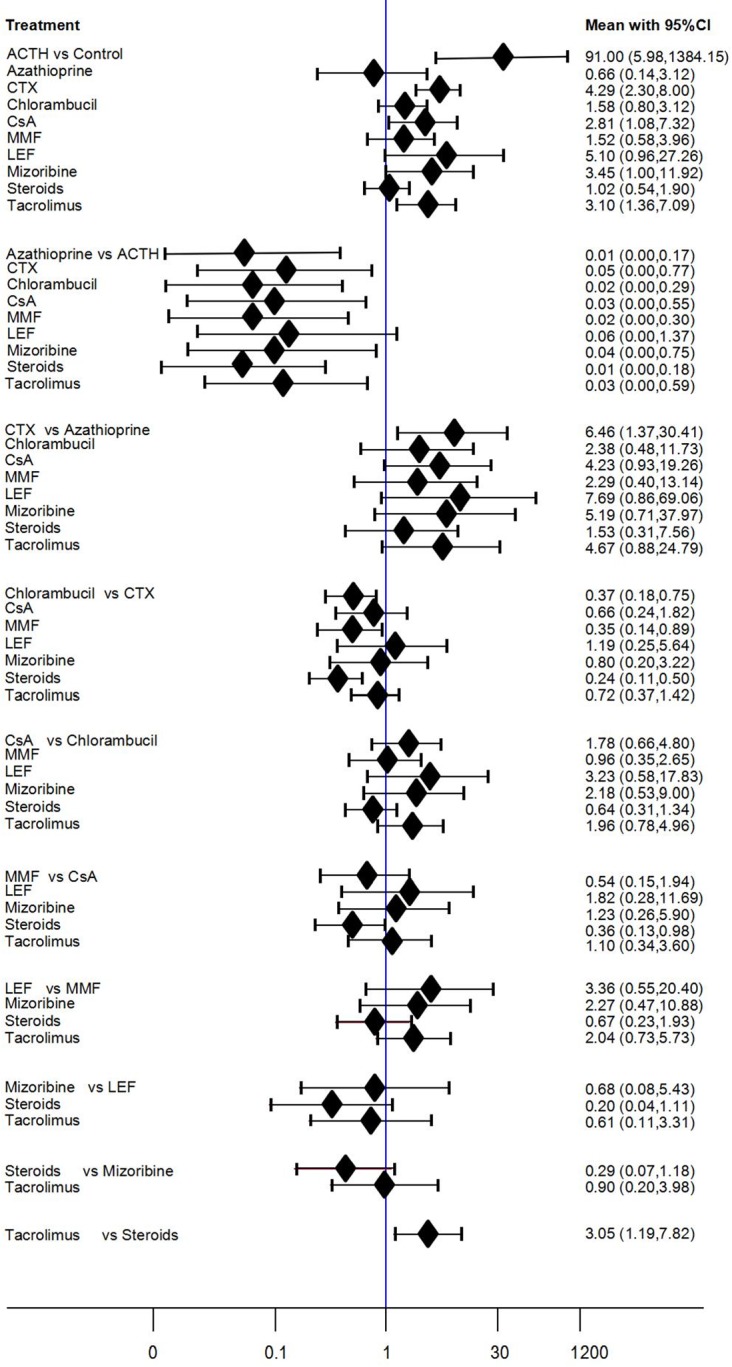
Total 36 randomized controlled trials (n = 2018) covering 11 kinds of treatments were included. Compared with non-immunosuppressive treatment, only cyclophosphamide (CTX) and chlorambucil significantly reduced the risk of composite outcome of mortality or ESKD while combining the direct and indirect comparison (OR = 0.31, 95%CI: 0.12-0.81 and OR = 0.33, 95%CI: 0.12-0.92). CTX increased the composite outcome of complete remission (CR) or partial remission (PR) (OR = 4.29, 95%CI: 2.30-8.00) but chlorambucil did not (OR = 1.58, 95%CI: 0.80-3.12) as compared with non-immunosuppressive treatment. Chlorambucil also significantly increased the withdrawal risk (OR = 3.34, 95%CI: 1.37-8.17) as compared to CTX. Both tacrolimus (OR = 3.10, 95%CI: 1.36-7.09) and cyclosporine (CsA) (OR = 2.81, 95%CI: 1.08-7.32) also significantly increased the rate of CR or PR as compared with non-immunosuppressive treatment (without significant difference as compared with CTX), while ranking results showed that cyclosporine or tacrolimus was with less possibility of drug withdrawal as compared to CTX.
Cyclophosphamide and chlorambucil reduce risk of ESKD or death in IMN with nephrotic range proteinuria, but carry substantial toxicity that may be lower for cyclophosphamide. Tacrolimus and cyclosporine increase the possibility of proteinuria remission with less drug withdrawal, but the effects on kidney failure remain uncertain.
一般而言,免疫抑制剂可预防患有肾病综合征的特发性膜性肾病(IMN)患者的肾脏病变进展及全因死亡率。然而,不同免疫抑制治疗的疗效和安全性尚未得到系统评估和比较。本研究进行了一项网状Meta分析,以比较IMN的不同免疫抑制治疗。
检索Cochrane图书馆、MEDLINE、EMBASE及试验注册系统,查找截至2016年5月3日报告IMN治疗的随机对照试验。采用网状Meta分析,结合直接和间接比较,比较死亡率或终末期肾病(ESKD)、完全或部分蛋白尿缓解以及因治疗不良事件而停药的复合终点。使用累积排序曲线下面积(SUCRA)分析不同免疫抑制治疗在各结局中的排名。
共纳入36项随机对照试验(n = 2018),涵盖11种治疗方法。与非免疫抑制治疗相比,仅环磷酰胺(CTX)和苯丁酸氮芥在结合直接和间接比较时,显著降低了死亡率或ESKD复合结局的风险(OR = 0.31,95%CI:0.12 - 0.81;OR = 0.33,95%CI:0.12 - 0.92)。与非免疫抑制治疗相比,CTX增加了完全缓解(CR)或部分缓解(PR)的复合结局(OR = 4.29,95%CI:2.30 - 8.00),但苯丁酸氮芥未增加(OR = 1.58,95%CI:0.80 - 3.12)。与CTX相比,苯丁酸氮芥也显著增加了停药风险(OR = 3.34,95%CI:1.37 - 8.17)。与非免疫抑制治疗相比,他克莫司(OR = 3.10,95%CI:1.36 - 7.09)和环孢素(CsA)(OR = 2.81,95%CI:1.08 - 7.32)也显著增加了CR或PR率(与CTX相比无显著差异),而排名结果显示,与CTX相比,环孢素或他克莫司停药的可能性较小。
环磷酰胺和苯丁酸氮芥可降低伴有肾病范围蛋白尿的IMN患者发生ESKD或死亡的风险,但具有较大毒性,环磷酰胺的毒性可能较低。他克莫司和环孢素增加了蛋白尿缓解的可能性且停药较少,但对肾衰竭的影响仍不确定。