Department of Intensive Care, Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
Department of Neurology, Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
J Intensive Care Med. 2020 Feb;35(2):161-169. doi: 10.1177/0885066617732747. Epub 2017 Sep 22.
Guidelines on the management of aneurysmal subarachnoid hemorrhage (aSAH) recommend euvolemia, whereas hypervolemia may cause harm. We investigated whether high early fluid input is associated with delayed cerebral ischemia (DCI), and if fluid input can be safely decreased using transpulmonary thermodilution (TPT).
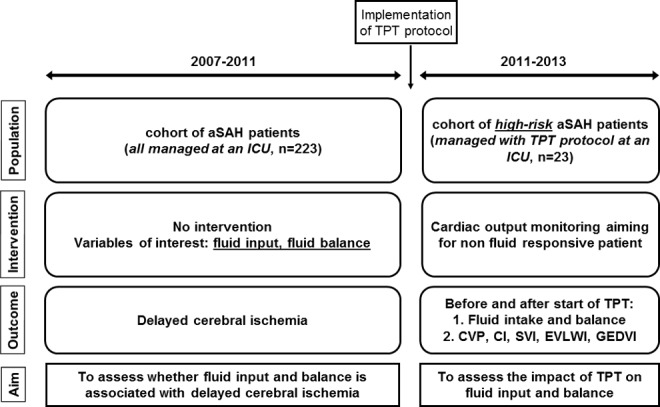
We retrospectively included aSAH patients treated at an academic intensive care unit (2007-2011; cohort 1) or managed with TPT (2011-2013; cohort 2). Local guidelines recommended fluid input of 3 L daily. More fluids were administered when daily fluid balance fell below +500 mL. In cohort 2, fluid input in high-risk patients was guided by cardiac output measured by TPT per a strict protocol. Associations of fluid input and balance with DCI were analyzed with multivariable logistic regression (cohort 1), and changes in hemodynamic indices after institution of TPT assessed with linear mixed models (cohort 2).
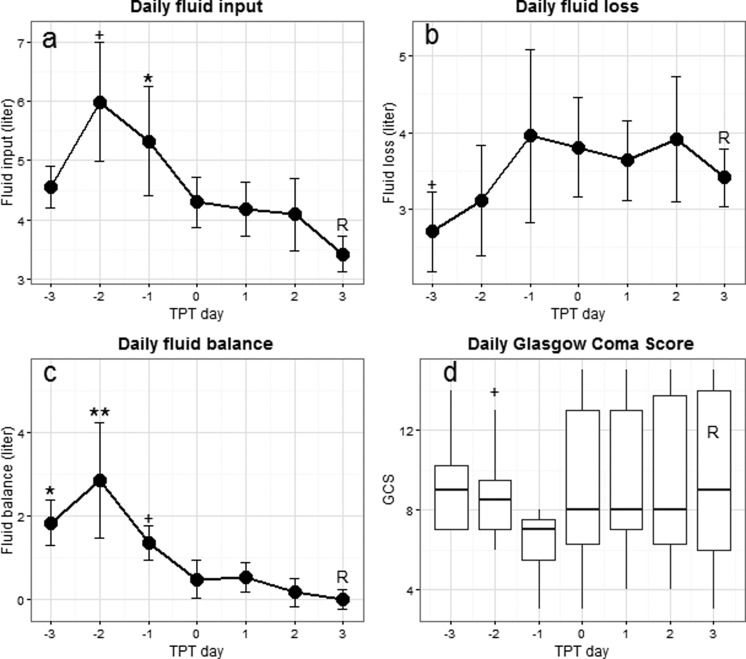
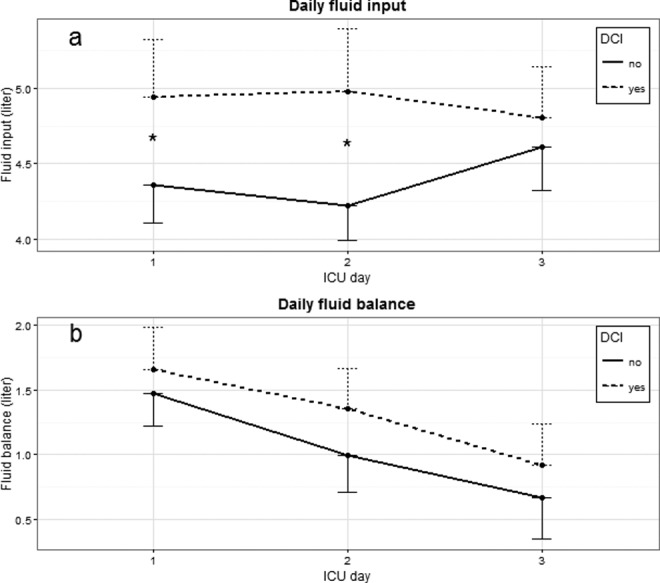
Cumulative fluid input 0 to 72 hours after admission was associated with DCI in cohort 1 (n=223; odds ratio [OR] 1.19/L; 95% confidence interval 1.07-1.32), whereas cumulative fluid balance was not. In cohort 2 (23 patients), using TPT fluid input could be decreased from 6.0 ± 1.0 L before to 3.4 ± 0.3 L; = .012), while preload parameters and consciousness remained stable.
High early fluid input was associated with DCI. Invasive hemodynamic monitoring was feasible to reduce fluid input while maintaining preload. These results indicate that fluid loading beyond a normal preload occurs, may increase DCI risk, and can be minimized with TPT.
关于蛛网膜下腔出血(aSAH)管理的指南建议血容量正常,而血容量过多可能会造成伤害。我们研究了早期高液体输入是否与迟发性脑缺血(DCI)相关,以及是否可以使用经肺热稀释(TPT)安全减少液体输入。
我们回顾性纳入了在学术性重症监护病房接受治疗的 aSAH 患者(2007-2011 年;队列 1)或接受 TPT 治疗的患者(2011-2013 年;队列 2)。当地指南建议每日液体输入量为 3 L。当每日液体平衡低于+500 mL 时,会给予更多的液体。在队列 2 中,高危患者的液体输入由 TPT 测量的每搏量指导,遵循严格的方案。使用多变量逻辑回归分析了队列 1 中液体输入和平衡与 DCI 的相关性,并使用线性混合模型评估了 TPT 实施后血流动力学指数的变化(队列 2)。
队列 1(n=223)中,入院后 0-72 小时的累积液体输入与 DCI 相关(优势比[OR]1.19/L;95%置信区间 1.07-1.32),而累积液体平衡与 DCI 不相关。在队列 2(23 例患者)中,使用 TPT 可将液体输入从 6.0±1.0 L 降低至 3.4±0.3 L;P=0.012),同时前负荷参数和意识状态保持稳定。
早期高液体输入与 DCI 相关。侵入性血流动力学监测可在维持前负荷的情况下减少液体输入。这些结果表明,存在超过正常前负荷的液体加载,可能增加 DCI 风险,并且可以通过 TPT 最小化。