Fidler Mary Jo, Frankenberger Casey, Seto Richard, Lobato Gabriela C, Fhied Cristina L, Sayidine Selina, Basu Sanjib, Pool Mark, Karmali Reem, Batus Marta, Lie Wen-Rong, Hayes David, Mistry Jehangir, Bonomi Philip, Borgia Jeffrey A
Section of Medical Oncology, Rush University Medical Center, Chicago, IL 60612, USA.
Pathology, Rush University Medical Center, Chicago, IL 60612, USA.
Oncotarget. 2017 Apr 28;8(35):58108-58121. doi: 10.18632/oncotarget.17510. eCollection 2017 Aug 29.
The objective of this study was to identify serum biomarkers capable of predicting clinical outcomes in previously-treated NSCLC patients with wild-type for EGFR activating mutations or insufficient tissue for mutation status determination.
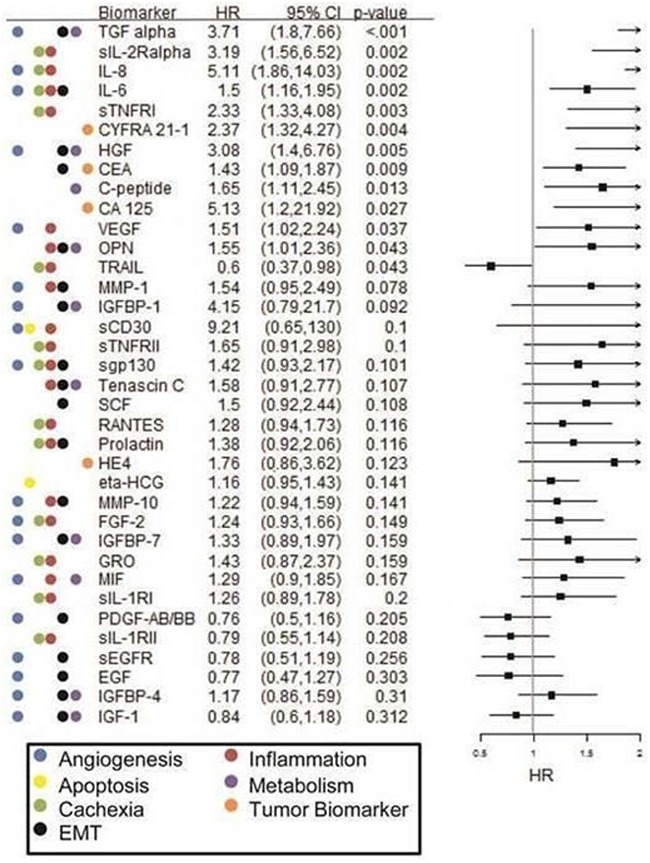
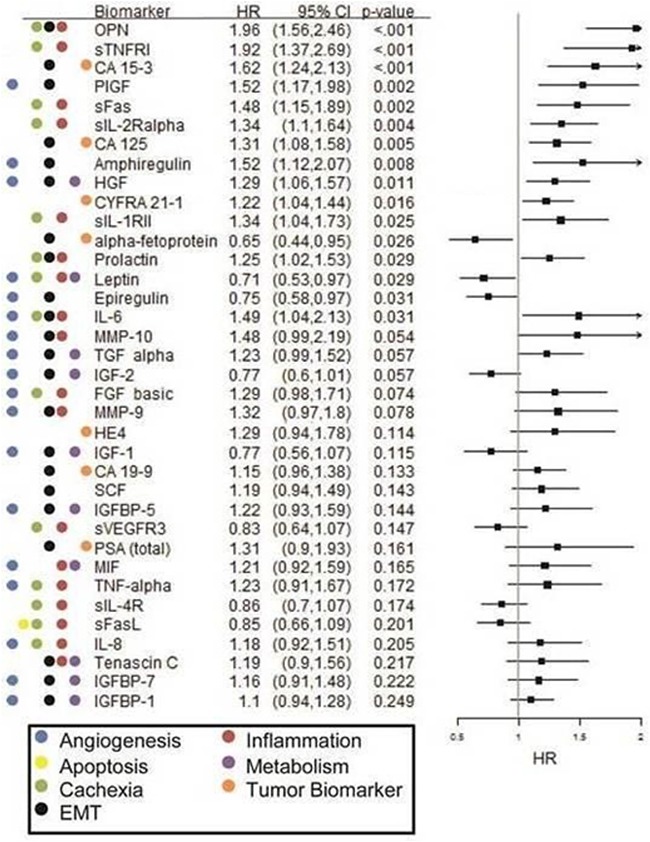
Sixty-six Luminex immunoassays representative of biological themes that emerged from a re-analysis of transcriptome data from the Cancer Genome Atlas (TCGA) were evaluate against pretreatment serum specimens from previously-treated advanced NSCLC patients received either cytotoxic chemotherapy (n=32) or erlotinib (n=79). Known EGFR mutation positive cases were excluded from analysis. Associations of biomarkers with outcome parameters and their differential interaction with treatment for survival outcomes were assessed using multivariate Cox PH analyses.
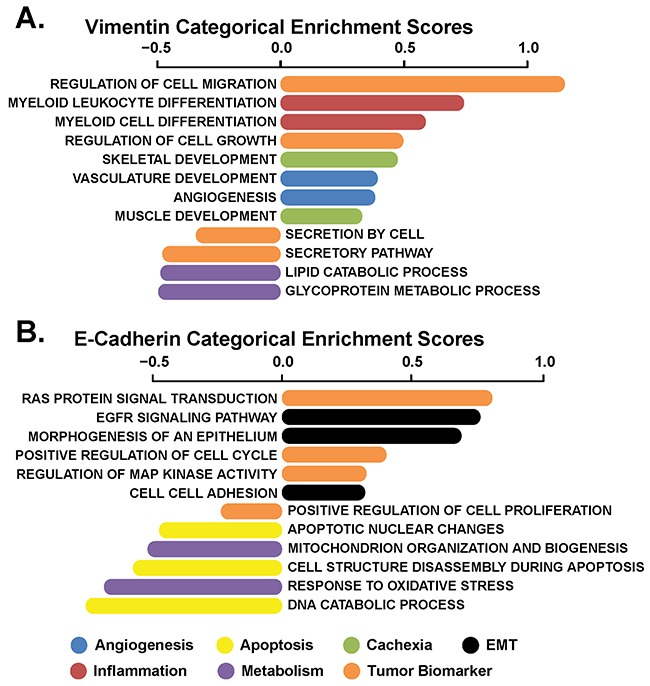
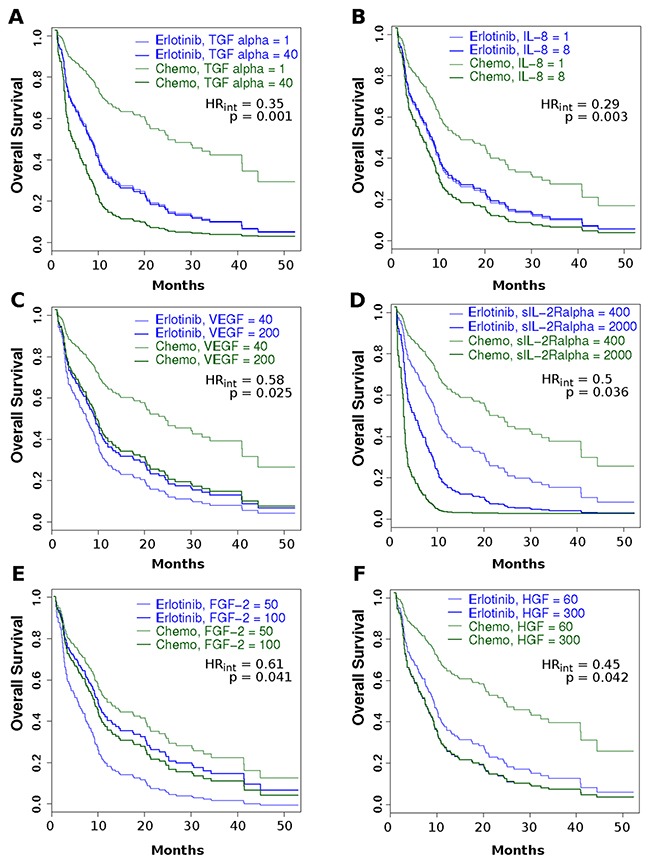
Our EMT-based transcriptomic analysis revealed a range of biological processes associated with angiogenesis, apoptosis, cachexia, inflammation, and metabolism emerging as those most highly associated with patient outcome. These processes were evaluated via surrogate serum biomarkers. A treatment-biomarker interaction analysis revealed that higher pretreatment levels of c-Met signaling biomarkers (i.e. HGF levels), pro-inflammatory/ pro-cachexia (e.g. IL-8, sIL-2Rα, FGF-2) processes and a pro-angiogenic (e.g. TGF-α, IL-8, VEGF) milieu were associated with inferior survival (HR=0.35, 0.29, 0.58, 0.50, 0.61, 0.45, respectively; all p<0.05) for patients receiving chemotherapy, relative to erlotinib. In contrast, high levels of decoy receptor for IL-1, sIL-1RII, and a high tissue vimentin/E-cadherin ratio were associated with a poor OS (HR=3.78; p=0.00055) in the erlotinib cohort.
Contemporary precision medicine initiatives that pair patient tumor characteristics with the optimal therapy type may maximize the use of agents targeting EGFR in the treatment of NSCLC.
本研究的目的是确定能够预测既往接受治疗的表皮生长因子受体(EGFR)激活突变野生型或组织不足以确定突变状态的非小细胞肺癌(NSCLC)患者临床结局的血清生物标志物。
针对来自癌症基因组图谱(TCGA)转录组数据重新分析中出现的生物学主题的66种Luminex免疫分析,对接受细胞毒性化疗(n = 32)或厄洛替尼(n = 79)治疗的既往接受治疗的晚期NSCLC患者的预处理血清标本进行评估。已知EGFR突变阳性病例被排除在分析之外。使用多变量Cox PH分析评估生物标志物与结局参数的关联及其与生存结局治疗的差异相互作用。
我们基于上皮-间质转化(EMT)的转录组分析揭示了一系列与血管生成、细胞凋亡、恶病质、炎症和代谢相关的生物学过程,这些过程与患者结局高度相关。这些过程通过替代血清生物标志物进行评估。治疗-生物标志物相互作用分析显示,与接受厄洛替尼治疗的患者相比,接受化疗的患者中,c-Met信号生物标志物(即肝细胞生长因子[HGF]水平)、促炎/促恶病质(如白细胞介素-8[IL-8]、可溶性白细胞介素-2受体α[sIL-2Rα]、成纤维细胞生长因子-2[FGF-2])过程和促血管生成(如转化生长因子-α[TGF-α]、IL-8、血管内皮生长因子[VEGF])环境的预处理水平较高与较差的生存率相关(风险比[HR]分别为0.35、0.29、0.58、0.50、0.61、0.45;均p<0.05)。相比之下,在厄洛替尼队列中,白细胞介素-1的诱饵受体sIL-1RII水平高以及组织波形蛋白/上皮钙黏蛋白比值高与较差的总生存期(OS)相关(HR = 3.78;p = 0.00055)。
将患者肿瘤特征与最佳治疗类型相结合的当代精准医学举措可能会最大限度地利用靶向EGFR的药物治疗NSCLC。