Università degli Studi and IRCCS Azienda Ospedaliera Universitaria San Martino-IST, Genova, Italy.
Department of Medical Sciences, Scientific Institute "Casa Sollievo della Sofferenza", San Giovanni Rotondo (FG), Italy.
J Am Heart Assoc. 2017 Sep 22;6(9):e006745. doi: 10.1161/JAHA.117.006745.
Apparent treatment resistant hypertension (aTRH) is highly prevalent in patients with type 2 diabetes mellitus (T2D) and entails worse cardiovascular prognosis. The impact of aTRH and long-term achievement of recommended blood pressure (BP) values on renal outcome remains largely unknown. We assessed the role of aTRH and BP on the development of chronic kidney disease in patients with T2D and hypertension in real-life clinical practice.
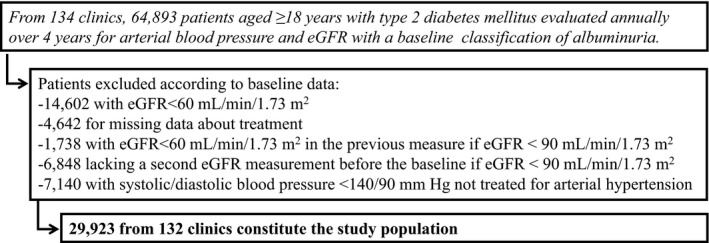
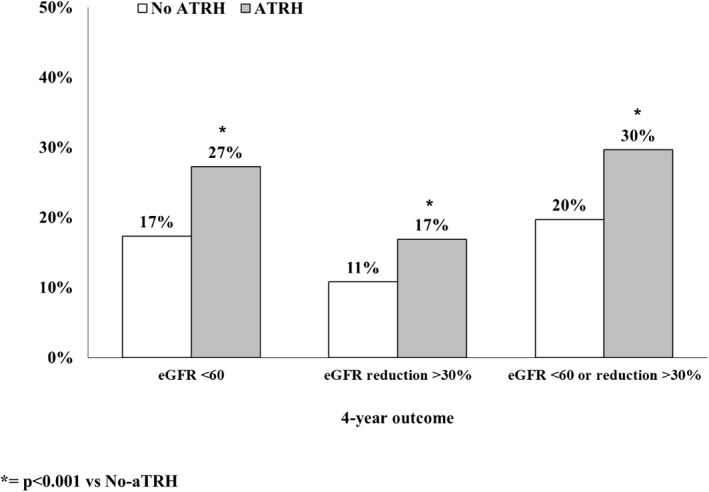
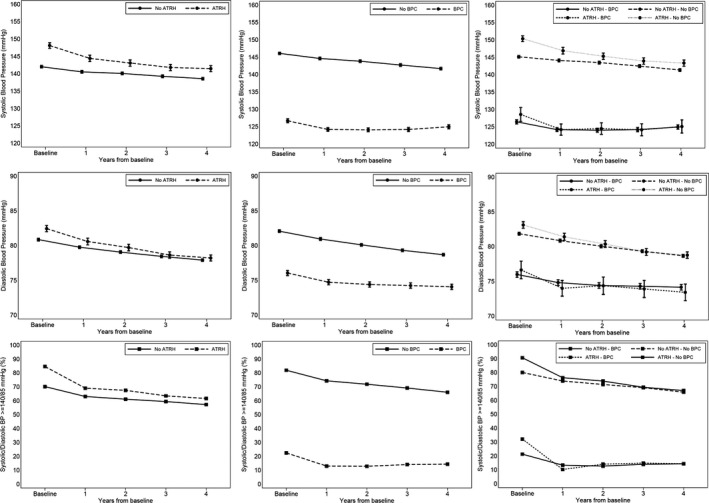
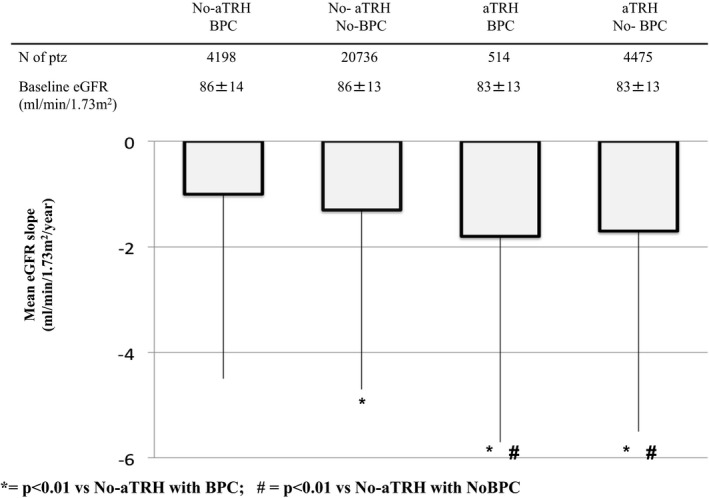
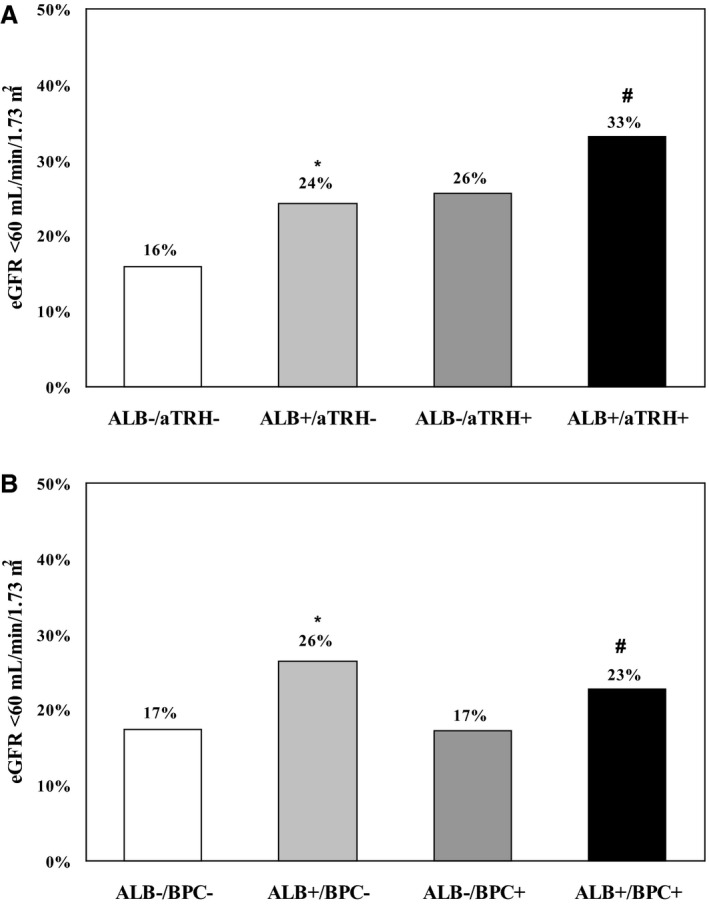
Clinical records from a total of 29 923 patients with T2D and hypertension, with normal baseline estimated glomerular filtration rate and regular visits during a 4-year follow-up, were retrieved and analyzed. The association between time-updated BP control (ie, 75% of visits with BP <140/90 mm Hg) and the occurrence of estimated glomerular filtration rate <60 and/or a reduction ≥30% from baseline was assessed. At baseline, 17% of patients had aTRH. Over the 4-year follow-up, 19% developed low estimated glomerular filtration rate and 12% an estimated glomerular filtration rate reduction ≥30% from baseline. Patients with aTRH showed an increased risk of developing both renal outcomes (adjusted odds ratio, 1.31 and 1.43; <0.001 respectively), as compared with those with non-aTRH. No association was found between BP control and renal outcomes in non-aTRH, whereas in aTRH, BP control was associated with a 30% (=0.036) greater risk of developing the renal end points.
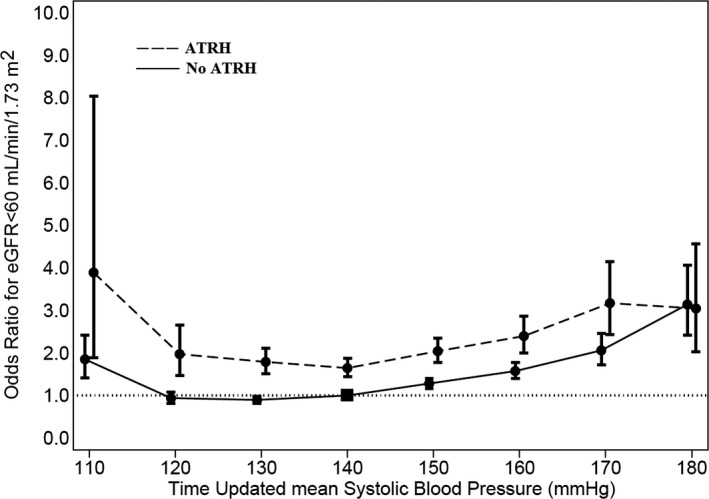
ATRH entails a worse renal prognosis in T2D with hypertension. BP control is not associated with a more-favorable renal outcome in aTRH. The relationship between time-updated BP and renal function seems to be J-shaped, with optimal systolic BP values between 120 and 140 mm Hg.
在 2 型糖尿病(T2D)患者中,明显的治疗抵抗性高血压(aTRH)患病率很高,并且对心血管预后有更差的影响。aTRH 和长期达到推荐的血压(BP)值对肾脏结局的影响在很大程度上仍然未知。我们评估了在真实临床实践中,aTRH 和 BP 在 T2D 合并高血压患者中发生慢性肾脏病的作用。
共检索并分析了 29923 例 T2D 合并高血压患者的临床记录,这些患者基线时估算肾小球滤过率正常,并且在 4 年随访期间定期就诊。评估了时间更新的 BP 控制(即,75%的就诊时 BP<140/90mmHg)与估算肾小球滤过率<60 和/或从基线下降≥30%的发生之间的关系。基线时,17%的患者有 aTRH。在 4 年的随访期间,19%的患者发生估算肾小球滤过率降低,12%的患者从基线下降≥30%。与非-aTRH 患者相比,aTRH 患者发生这两种肾脏结局的风险增加(调整后的优势比分别为 1.31 和 1.43;均<0.001)。在非-aTRH 患者中,BP 控制与肾脏结局之间没有关联,而在 aTRH 中,BP 控制与发生肾脏终点的风险增加 30%(=0.036)相关。
在 T2D 合并高血压患者中,aTRH 预示着更差的肾脏预后。BP 控制与 aTRH 患者的肾脏结局无相关性。时间更新的 BP 与肾功能之间的关系呈 J 型,最佳收缩压值在 120-140mmHg 之间。