Zhang Fan, Kanzali Parisa, Rubin Vadim, Paras Chris, Goldman Joel
Department of Internal Medicine, Brookdale University Hospital and Medical Center, Brooklyn Ross University School of Medicine, Portsmouth, Dominica Division of Endocrinology, Brookdale University Hospital and Medical Center, Brooklyn, New York.
Medicine (Baltimore). 2017 Sep;96(39):e8191. doi: 10.1097/MD.0000000000008191.
Neuroleptic malignant syndrome (NMS) is a life threatening neurologic emergency associated with neuroleptic or antipsychotic agent use. NMS is rarely related to thyroid disease.
We report a case of NMS in a 66-year-old male with past medical history of paranoid schizophrenia on chlorpromazine, diabetes, hypertension and asthma, who presented with a humeral fracture after a fall. Patient developed hyperpyrexia, altered consciousness, autonomic instability, elevated serum creatine kinase (CK) without rigidity.
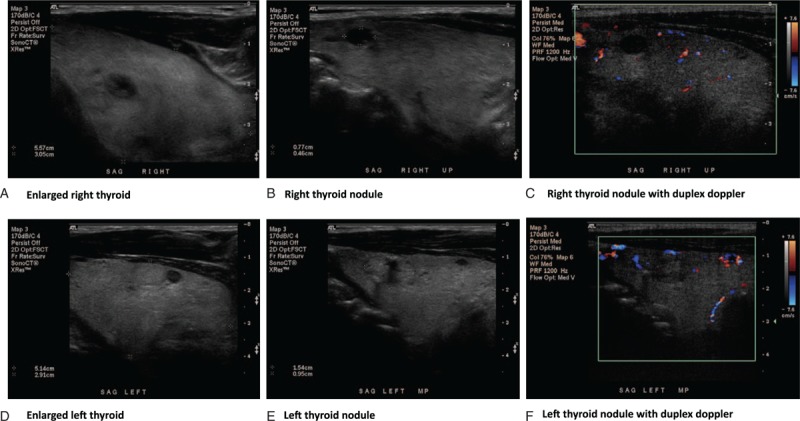
CT head and workup for infection were negative. Electroencephalogram (EEG) showed generalized slow wave activity. Ultrasound revealed a large goiter with nodules.
Chlorpromazine was stopped due to concern of NMS. Patient was treated with cooling, fluid and electrolyte maintenance.
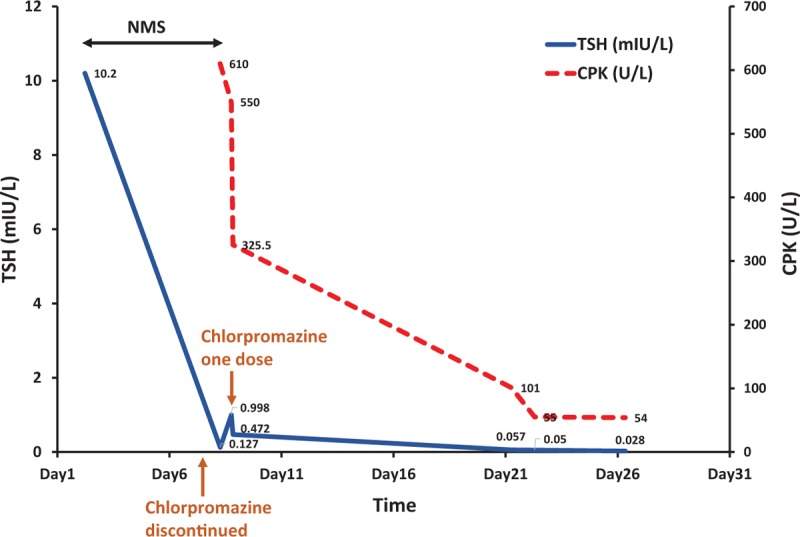
Patient slowly improved and CK level normalized. Thyroid-stimulating hormone (TSH) level trended down from 10.2 mIU/L to 0.02 mIU/L. Patient was discharged with aripiprazole.
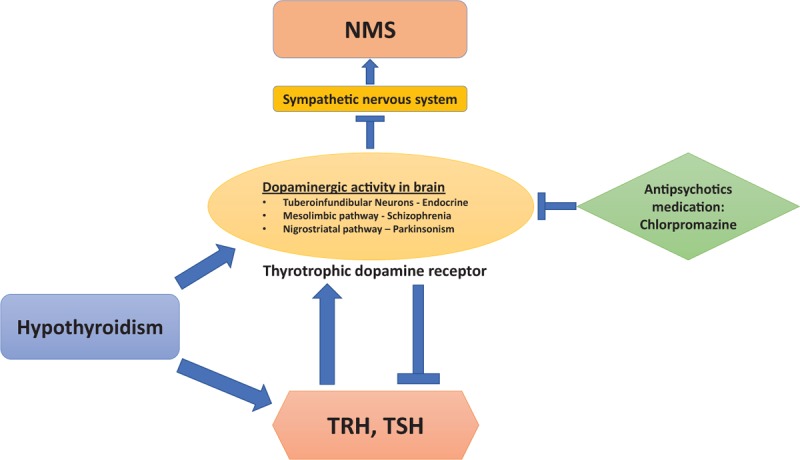
Hypothyroidism predisposes patients to NMS by altering central dopaminergic systems. The typical symptoms may be masked by hypothyroidism. Thyroid dysfunction should be excluded in all patients with NMS. Discontinuing antipsychotic agents decreases TSH levels which maybe due to the negative feedback of dopaminergic activity. This is the first case report describing dramatic changes in TSH after discontinuing chlorpromazine in NMS.
抗精神病药物恶性综合征(NMS)是一种与使用抗精神病药物相关的危及生命的神经急症。NMS很少与甲状腺疾病相关。
我们报告一例66岁男性NMS病例,该患者有偏执型精神分裂症病史,正在服用氯丙嗪,同时患有糖尿病、高血压和哮喘,因跌倒导致肱骨骨折。患者出现高热、意识改变、自主神经功能不稳定、血清肌酸激酶(CK)升高但无强直。
头颅CT及感染相关检查均为阴性。脑电图(EEG)显示广泛性慢波活动。超声检查发现一个伴有结节的大甲状腺肿。
因担心NMS而停用氯丙嗪。患者接受了降温、液体和电解质维持治疗。
患者逐渐好转,CK水平恢复正常。促甲状腺激素(TSH)水平从10.2 mIU/L降至0.02 mIU/L。患者出院时服用阿立哌唑。
甲状腺功能减退通过改变中枢多巴胺能系统使患者易患NMS。典型症状可能被甲状腺功能减退掩盖。所有NMS患者均应排除甲状腺功能障碍。停用抗精神病药物会降低TSH水平,这可能是由于多巴胺能活性的负反馈作用。这是首例描述NMS患者停用氯丙嗪后TSH发生显著变化的病例报告。