Department of Interventional Neuroradiology, West Virginia University Hospital, Morgantown, West Virginia, USA.
Department of Enterprise Analytics, West Virginia University Hospital, Morgantown, West Virginia, USA.
J Neurointerv Surg. 2018 Jun;10(6):510-515. doi: 10.1136/neurintsurg-2017-013371. Epub 2017 Sep 28.
M2 occlusions may result in poor outcomes and potentially benefit from endovascular therapy. Data on the rate of M2 strokes is lacking.
Patients with acute ischemic stroke discharged over a period of 3 years from a tertiary level hospital in the 'stroke belt' were evaluated for M2 occlusions on baseline vascular imaging. Regional and national incidence was calculated from discharge and multicounty data.
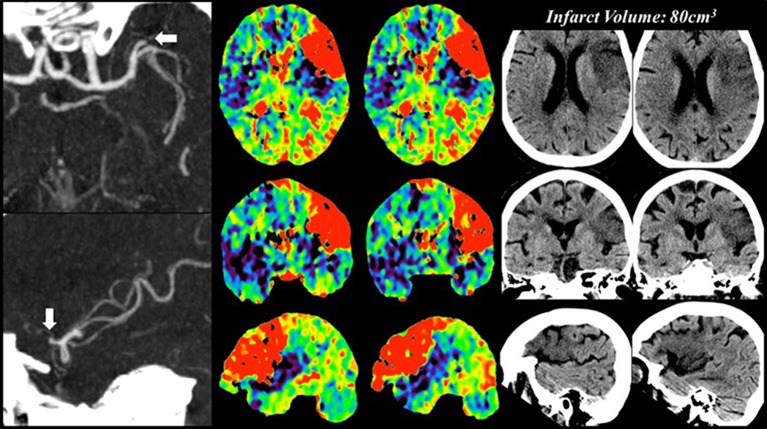
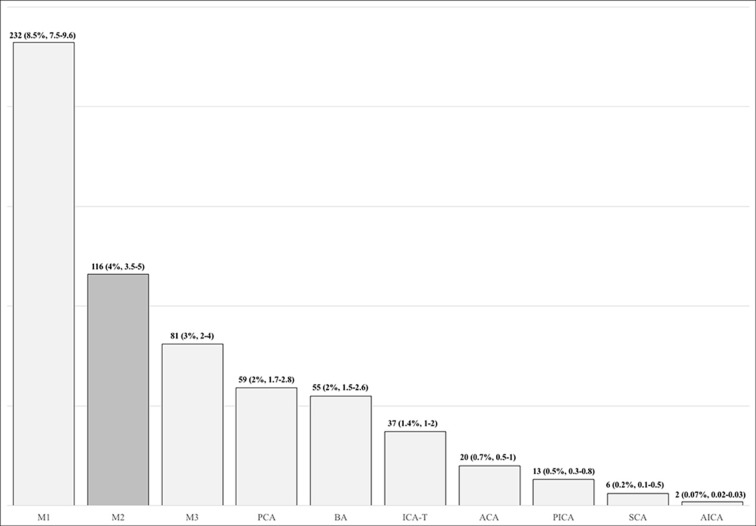
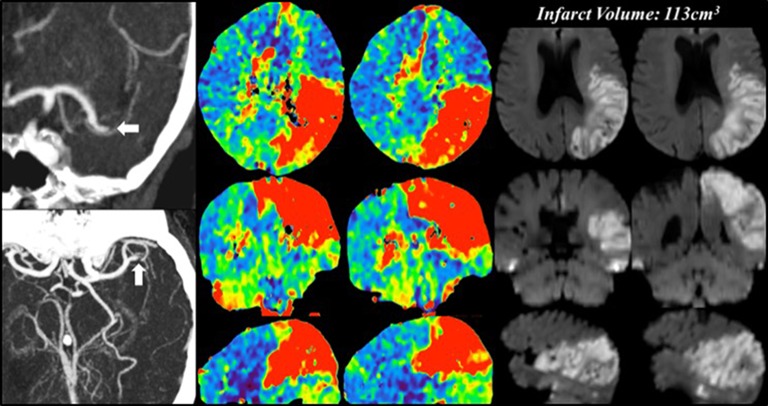
There were 2739 ICD-9 based AIS discharges. M2 occlusions in 116 (4%, 95% CI 3.5% to 5%) patients constituted the second most common occlusion site. The median National Institute of Health Stroke Scale (NIHSS) score was 12 (IQR 5-18). Good outcomes were observed in 43% (95% CI 34% to 53%), poor outcomes in 57% (95% CI 47% to 66%), and death occurred in 27% (95% CI 19% to 37%) of patients. Receiver operating characteristics curves showed the NIHSS to be predictive of outcomes (area under the curve 0.829, 95% CI 0.745 to 0.913, p<0.0001). An NIHSS score ≥9 was the optimal cut-off point for predicting poor outcomes (sensitivity 85.7%, specificity 67.4%). 71 (61%) patients had an NIHSS score ≥9 and 45 (39%) an NIHSS score <9. The rate of good-outcome was 22.6% for NIHSS score ≥9 versus 78.4% for NIHSSscore <9 (OR=0.08, 95% CI 0.03 to 0.21, p<0.0001). Mortality was 42% for NIHSS score ≥9 versus 2.7% for NIHSS score <9 (OR=26, 95% CI 3.3 to 202, p<0.0001). Infarct volume was 57 (±55.7) cm for NIHSS score ≥9 versus 30 (±34)cm for NIHSS score <9 (p=0.003). IV recombinant tissue plasminogen activator (rtPA) administered in 28 (24%) patients did not affect outcomes. The rate of M2 occlusions was 7 (95% CI 5 to 9)/100 000 people/year (3%, 95% CI 2% to 4%), giving an incidence of 21 176 (95% CI 15 282 to 29 247)/year. Combined with M1, internal carotid artery terminus and basilar artery, this yields a 'large vessel occlusion (LVO)+M2' rate of 31 (95% CI 26 to 35)/100 000 people/year and a national incidence of 99 227 (95% CI 84 004 to 112 005) LVO+M2 strokes/year.
M2 occlusions can present with serious neurological deficits and cause significant morbidity and mortality. Patients with M2 occlusions and higher baseline deficits (NIHSS score ≥9) may benefit from endovascular therapy, thus potentially expanding the category of acute ischemic strokes amenable to intervention.
M2 闭塞可能导致不良结局,并可能受益于血管内治疗。关于 M2 中风的发生率数据尚缺乏。
在“中风带”的一家三级医院,对在 3 年期间出院的急性缺血性中风患者进行基线血管成像评估 M2 闭塞。根据出院和多县数据计算区域和国家发病率。
共有 2739 例基于 ICD-9 的 AIS 出院。116 例(4%,95%CI 3.5%至 5%)患者存在 M2 闭塞,是第二常见的闭塞部位。中位数国立卫生研究院中风量表(NIHSS)评分为 12(IQR 5-18)。43%(95%CI 34%至 53%)的患者预后良好,57%(95%CI 47%至 66%)的患者预后不良,27%(95%CI 19%至 37%)的患者死亡。受试者工作特征曲线显示 NIHSS 可预测结局(曲线下面积 0.829,95%CI 0.745 至 0.913,p<0.0001)。NIHSS 评分≥9 是预测不良结局的最佳截断值(灵敏度 85.7%,特异性 67.4%)。71 例(61%)患者 NIHSS 评分≥9,45 例(39%)患者 NIHSS 评分<9。NIHSS 评分≥9 的良好结局率为 22.6%,NIHSS 评分<9 的为 78.4%(OR=0.08,95%CI 0.03 至 0.21,p<0.0001)。NIHSS 评分≥9 的死亡率为 42%,NIHSS 评分<9 的为 2.7%(OR=26,95%CI 3.3 至 202,p<0.0001)。NIHSS 评分≥9 的梗死体积为 57(±55.7)cm,NIHSS 评分<9 的为 30(±34)cm(p=0.003)。28 例(24%)患者接受了重组组织型纤溶酶原激活剂(rtPA)静脉溶栓治疗,但并未影响结局。M2 闭塞的发生率为 7(95%CI 5 至 9)/100 000 人/年(3%,95%CI 2%至 4%),发病率为 21 176(95%CI 15 282 至 29 247)/年。与 M1、颈内动脉终末段和基底动脉合并计算,“大血管闭塞(LVO)+M2”的发生率为 31(95%CI 26 至 35)/100 000 人/年,全国 LVO+M2 中风发病率为 99 227(95%CI 84 004 至 112 005)/年。
M2 闭塞可能导致严重的神经功能缺损,并导致显著的发病率和死亡率。M2 闭塞且基线缺损较高(NIHSS 评分≥9)的患者可能受益于血管内治疗,从而可能扩大适合干预的急性缺血性中风范围。