Menéndez Rosario, Méndez Raúl, Polverino Eva, Rosales-Mayor Edmundo, Amara-Elori Isabel, Reyes Soledad, Sahuquillo-Arce José Miguel, Fernández-Barat Laia, Alcaraz Victoria, Torres Antoni
Pneumology Department, Hospital Universitario y Politécnico La Fe / Instituto de Investigación Sanitaria (IIS) La Fe, Universidad de Valencia, Valencia, Spain.
Centro de Investigación Biomédica En Red-Enfermedades Respiratorias (CIBERES, CB06/06/0028), Madrid, Spain.
BMC Infect Dis. 2017 Sep 30;17(1):659. doi: 10.1186/s12879-017-2754-5.
Non-cystic fibrosis bronchiectasis is a chronic structural lung condition that courses with recurrent infectious exacerbations that lead to frequent antibiotic treatment making this population more susceptible to acquire pathogens with antibiotic resistance. We aimed to investigate risk factors associated with isolation of multidrug-resistant pathogens in bronchiectasis exacerbations.
A prospective observational study was conducted in two tertiary-care hospitals, enrolling patients when first exacerbation appeared. Multidrug-resistance was determined according to European Centre of Diseases Prevention and Control classification.
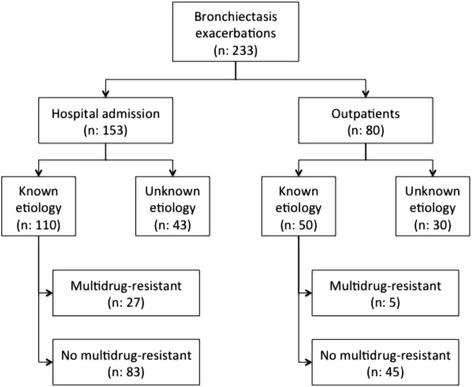
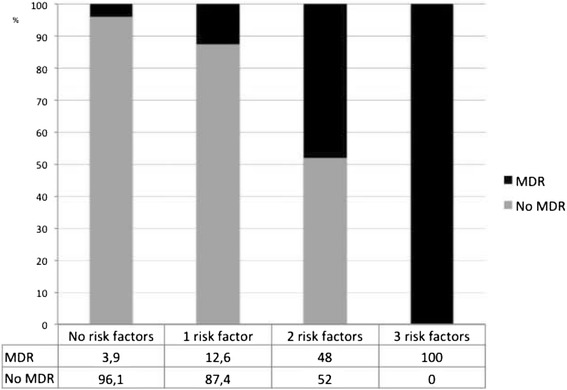
Two hundred thirty three exacerbations were included and microorganisms were isolated in 159 episodes. Multidrug-resistant pathogens were found in 20.1% episodes: Pseudomonas aeruginosa (48.5%), methicillin-resistant Staphylococcus aureus (18.2%) and Extended spectrum betalactamase + Enterobacteriaceae (6.1%), and they were more frequent in exacerbations requiring hospitalization (24.5% vs. 10.2%, p: 0.016). Three independent multidrug-resistant risk factors were found: chronic renal disease (Odds ratio (OR), 7.60, 95% CI 1.92-30.09), hospitalization in the previous year (OR, 3.88 95% CI 1.37-11.02) and prior multidrug-resistant isolation (OR, 5.58, 95% CI 2.02-15.46). The proportion of multidrug-resistant in the 233 exacerbations was as follows: 3.9% in patients without risk factors, 12.6% in those with 1 factor and 53.6% if ≥2 risk factors.
Hospitalization in the previous year, chronic renal disease, and prior multidrug-resistant isolation are risk factors for identification multidrug-resistant pathogens in exacerbations. This information may assist clinicians in choosing empirical antibiotics in daily clinical practice.
非囊性纤维化支气管扩张是一种慢性肺部结构性疾病,病程中伴有反复的感染加重,常需频繁使用抗生素治疗,这使得该人群更容易感染具有抗生素耐药性的病原体。我们旨在调查支气管扩张加重期与多重耐药病原体分离相关的危险因素。
在两家三级医院进行了一项前瞻性观察性研究,纳入首次出现加重期的患者。根据欧洲疾病预防控制中心的分类确定多重耐药情况。
共纳入233次加重期,159次分离出微生物。20.1%的加重期发现多重耐药病原体:铜绿假单胞菌(48.5%)、耐甲氧西林金黄色葡萄球菌(18.2%)和超广谱β-内酰胺酶+肠杆菌科(6.1%),在需要住院治疗的加重期更为常见(24.5%对10.2%,p:0.016)。发现了三个独立的多重耐药危险因素:慢性肾病(比值比(OR),7.60,95%可信区间1.92-30.09)、上一年住院(OR,3.88,95%可信区间1.37-11.02)和既往多重耐药菌分离(OR,5.58,95%可信区间2.02-15.46)。233次加重期中多重耐药的比例如下:无危险因素的患者为3.9%,有1个危险因素的患者为12.6%,有≥2个危险因素的患者为53.6%。
上一年住院、慢性肾病和既往多重耐药菌分离是加重期鉴定多重耐药病原体 的危险因素。这些信息可能有助于临床医生在日常临床实践中选择经验性抗生素。