Chang Yi-Sheng, Chen Po-Lin, Hung Jia-Horung, Chen Hsiao-Yen, Lai Chun-Chieh, Ou Chun-Yen, Chang Chia-Ming, Wang Chien-Kuo, Cheng Hon-Chun, Tseng Sung-Huei
Department of Ophthalmology, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
Department of Ophthalmology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
PLoS One. 2017 Oct 3;12(10):e0184477. doi: 10.1371/journal.pone.0184477. eCollection 2017.
Paranasal sinusitis is widespread and can lead to orbital complications, blindness, and death. However, the correlation between ophthalmological findings and disease staging remains unclear. This study aimed to investigate the staging, acute ophthalmological manifestations, diagnosis, management, and outcomes of orbital complications of paranasal sinusitis during a 27-year period.
We retrospectively reviewed the medical records of all patients with orbital complications of paranasal sinusitis hospitalized at the National Cheng Kung University Hospital, a medical center in Taiwan during 1988-2015. Sex, age, symptoms, history, ophthalmological findings, laboratory and imaging findings, treatments, and outcomes were analyzed by staging.
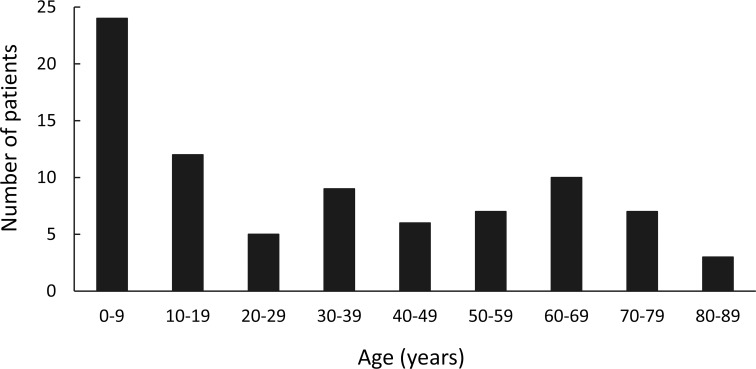
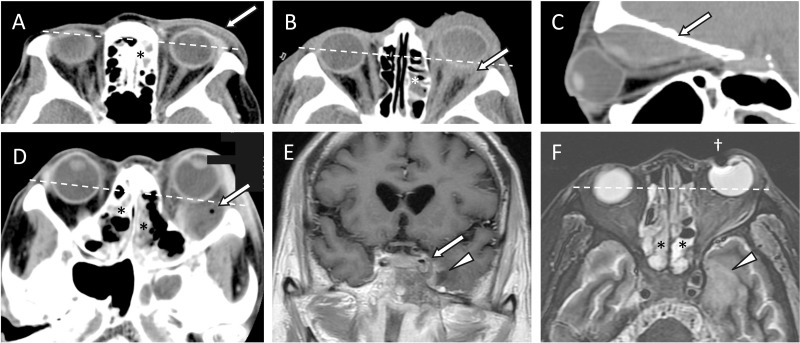
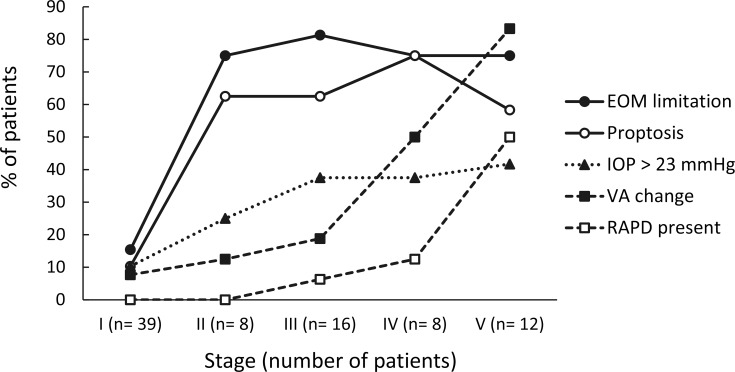
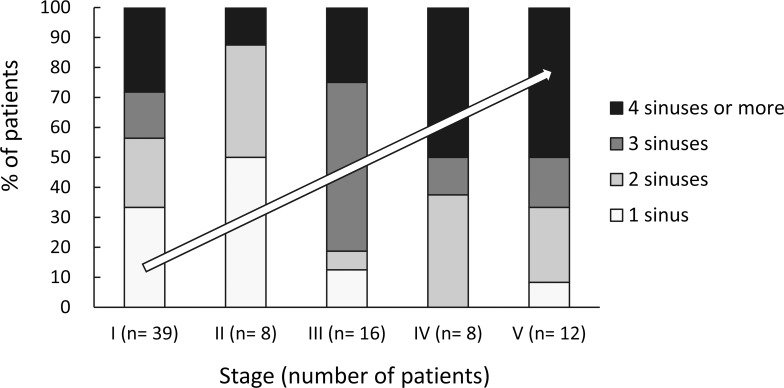
Eighty-three patients aged 9 days to 80 years had stage I (preseptal cellulitis, n = 39 patients), II (postseptal orbital cellulitis, n = 8), III (subperiosteal abscess, n = 16), IV (orbital abscess, n = 8), or V (intracranial involvement, n = 12) complications. Peak incidences occurred in patients aged 0-19 and 60-69 years. Chronic sinusitis and diabetes mellitus were common preexisting diseases. Extraocular movement limitation and proptosis predicted postseptal (stage II or more) involvement. The likelihood of elevated intraocular pressure increased with stage. Reduced visual acuity and presence of relative afferent pupillary defect indicated consideration of magnetic resonance imaging to investigate possible intracranial extension. Ipsilateral maxillary (81.7%) and ethmoidal (75.6%) sinuses were the most common sources of infection, and the most frequently implicated pathogens were coagulase-negative Staphylococcus spp. (25.3%) and Staphylococcus aureus (20.5%). All patients received intravenous antimicrobial therapy (multi-drug therapy in 88.0%), and 55.4% underwent surgery, most commonly endoscopic sinus surgery. One (1.2%) diabetic man with stage V complications died of fungal sinusitis with intracranial invasion. Five (6.0%) patients, all stage V, lost vision despite intensive treatment. The average length of hospital stay was 13.8 days (range 2-72 days), and significantly longer stays were associated with stages II-V as compared to stage I.
Orbital infection originating from paranasal sinusitis can cause vision loss and death due to intracranial extension. Acute ophthalmological findings predict staging and prognosis. Cooperative consultation between ophthalmologists, otorhinolaryngologists, and neurologists is essential. Urgent diagnostic studies and aggressive antimicrobial therapy are indicated, and surgery should be considered.
鼻窦炎很常见,可导致眼眶并发症、失明甚至死亡。然而,眼科检查结果与疾病分期之间的相关性仍不明确。本研究旨在调查27年间鼻窦炎眼眶并发症的分期、急性眼科表现、诊断、治疗及预后情况。
我们回顾性分析了1988年至2015年期间在台湾医学中心国立成功大学医院住院的所有鼻窦炎眼眶并发症患者的病历。按分期分析患者的性别、年龄、症状、病史、眼科检查结果、实验室及影像学检查结果、治疗方法及预后情况。
83例年龄在9天至80岁之间的患者出现了I期(眶隔前蜂窝织炎,39例)、II期(眶隔后蜂窝织炎,8例)、III期(骨膜下脓肿,16例)、IV期(眶脓肿,8例)或V期(颅内受累,12例)并发症。发病高峰出现在0至19岁和60至69岁的患者中。慢性鼻窦炎和糖尿病是常见的基础疾病。眼球运动受限和眼球突出提示眶隔后(II期或更晚期)受累。眼压升高的可能性随分期增加。视力下降和相对传入性瞳孔障碍提示应考虑行磁共振成像检查以评估是否存在颅内扩展。同侧上颌窦(81.7%)和筛窦(75.6%)是最常见的感染源,最常见的病原体是凝固酶阴性葡萄球菌属(25.3%)和金黄色葡萄球菌(20.5%)。所有患者均接受了静脉抗菌治疗(88.0%为联合用药),55.4%的患者接受了手术,最常见的是鼻内镜鼻窦手术。1例患有V期并发症的糖尿病男性患者死于真菌性鼻窦炎伴颅内侵犯。5例(6.0%)患者均为V期,尽管接受了积极治疗仍失明。平均住院时间为13.8天(2至72天),与I期相比,II至V期患者的住院时间明显更长。
源自鼻窦炎的眼眶感染可因颅内扩展导致视力丧失甚至死亡。急性眼科检查结果可预测分期及预后。眼科医生、耳鼻喉科医生和神经科医生之间的协作会诊至关重要。应进行紧急诊断检查并积极进行抗菌治疗,必要时应考虑手术治疗。