Montano Ryan, Khan Nadeem, Hou Huagang, Seigne John, Ernstoff Marc S, Lewis Lionel D, Eastman Alan
Department of Molecular and Systems Biology, Geisel School of Medicine at Dartmouth, Lebanon, NH, USA.
Department of Radiology, Geisel School of Medicine at Dartmouth, Lebanon, NH, USA.
Oncotarget. 2017 Jun 28;8(40):67754-67768. doi: 10.18632/oncotarget.18834. eCollection 2017 Sep 15.
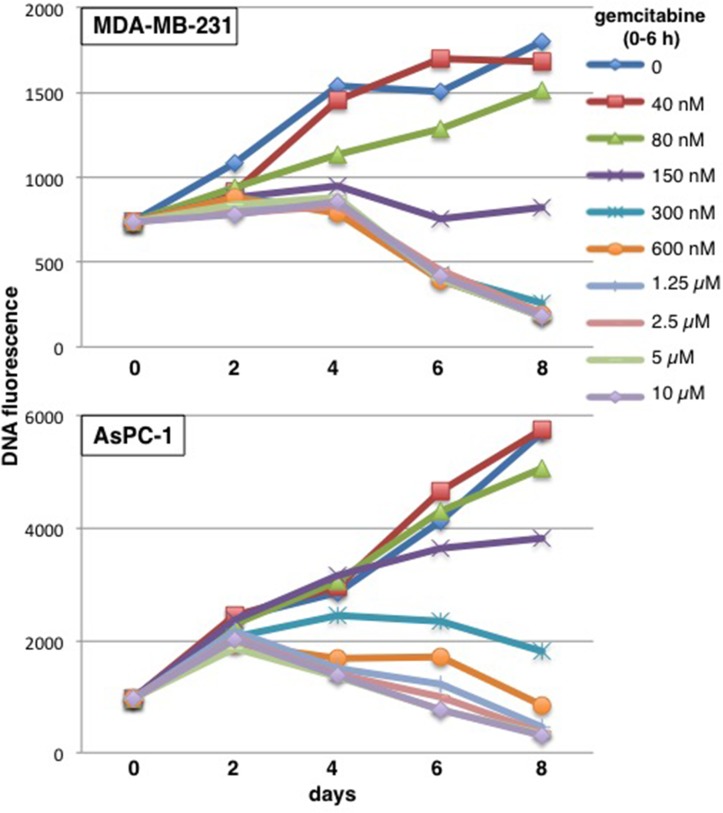
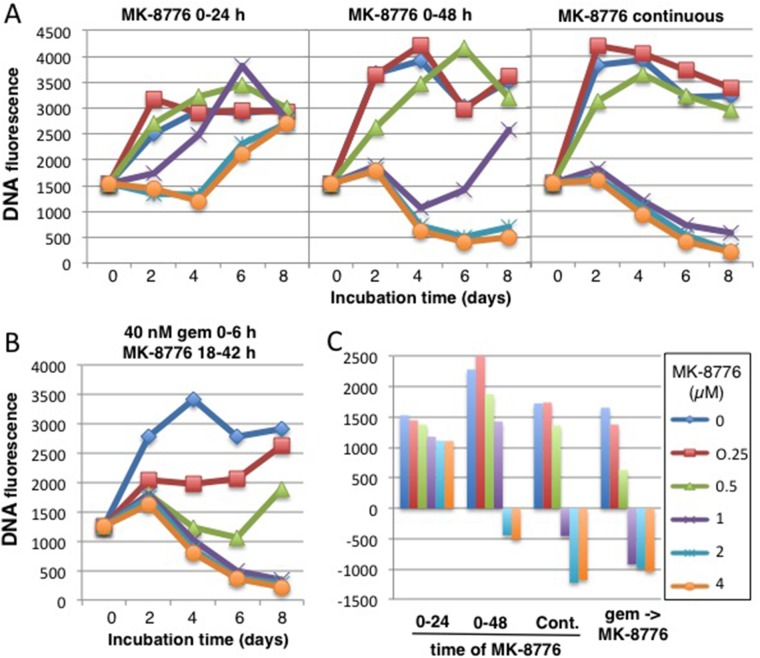
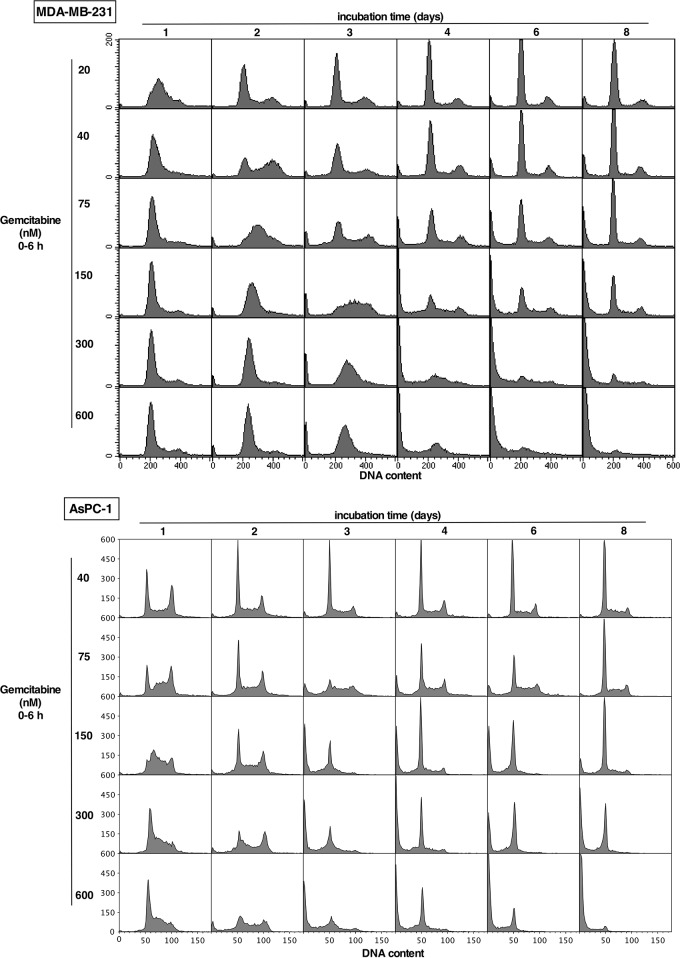
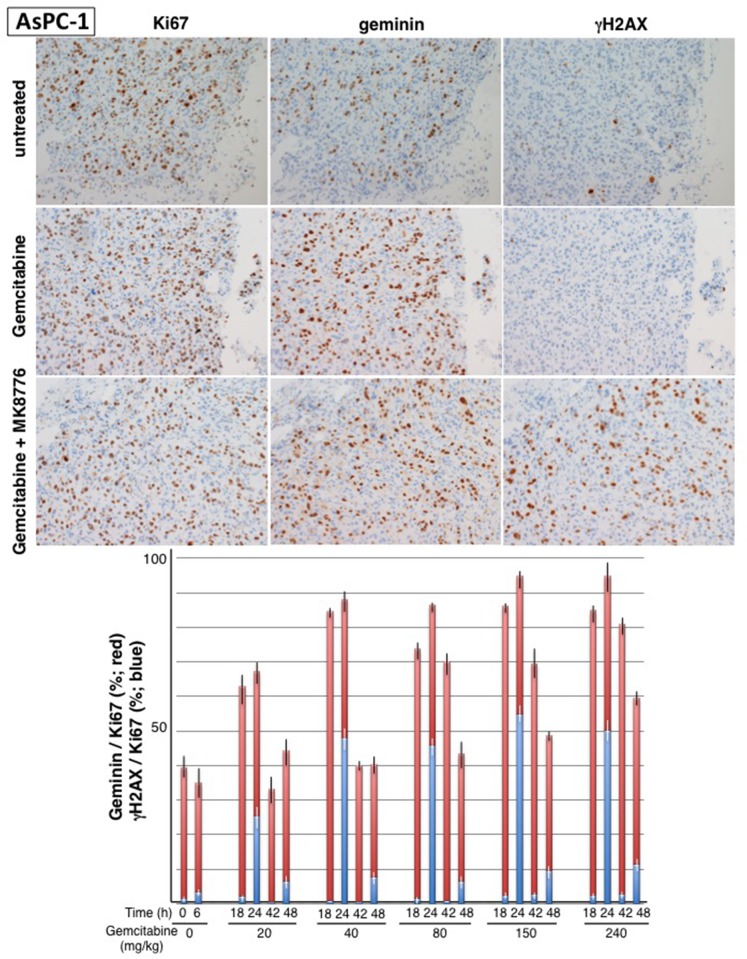
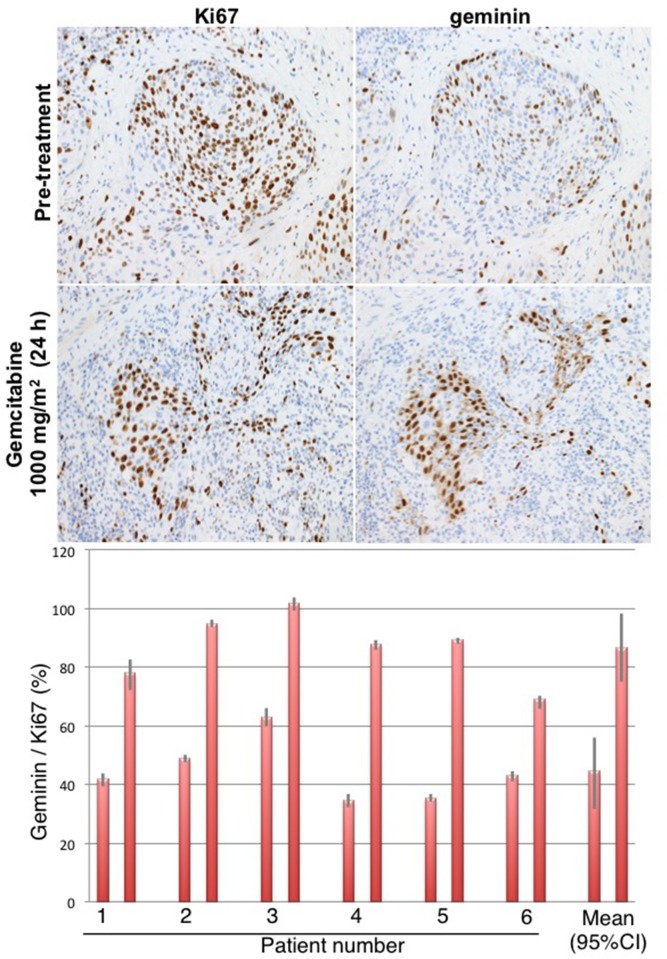
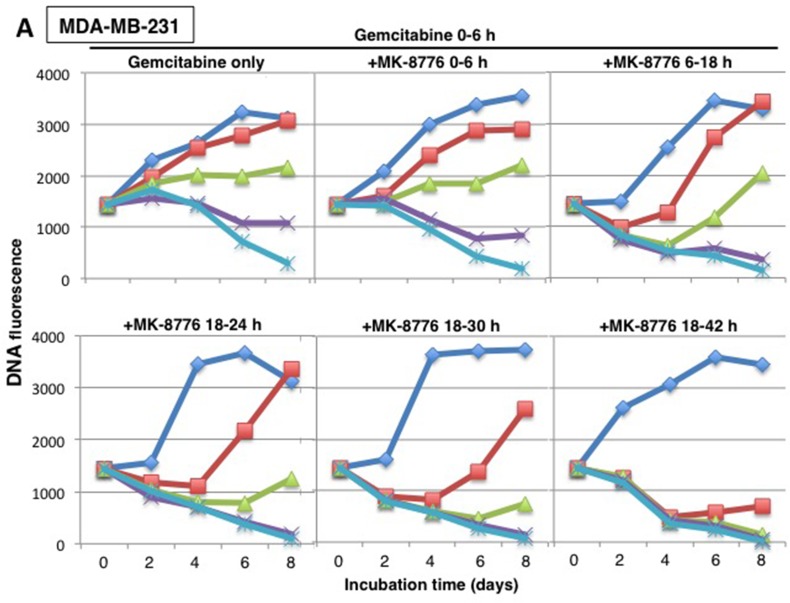
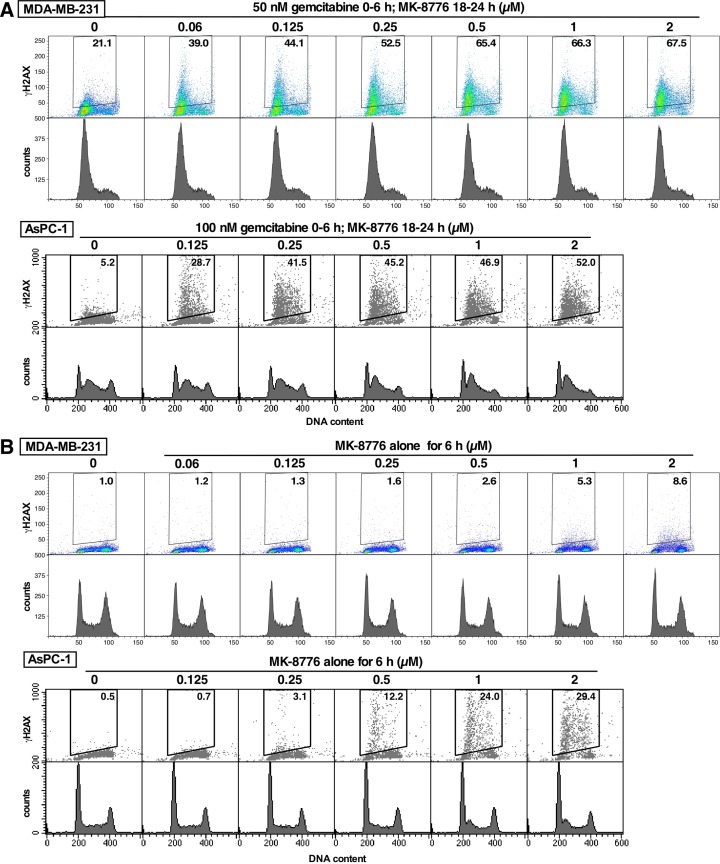
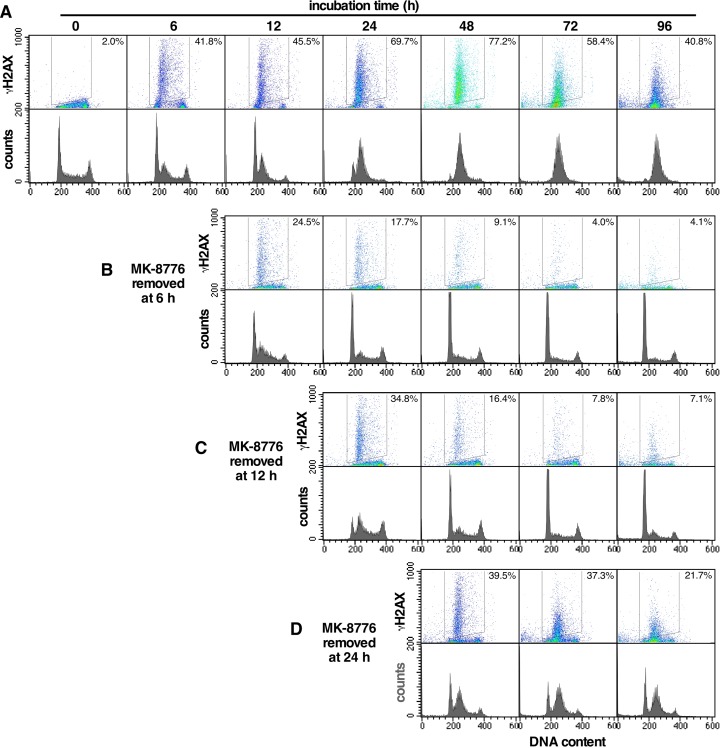
Gemcitabine irreversibly inhibits ribonucleotide reductase and induces S phase arrest but whether this occurs in tumors in mice or patients has not been established. Tumor cells in culture were incubated with gemcitabine for 6 h to approximate the administration schedule in a patient. Concentrations that induced persistent S phase arrest thereafter correlated with cell killing. Administration of gemcitabine to mice also demonstrated a persistent S phase arrest in their tumor. The minimum dose that induced almost complete S phase arrest after 24 h (40 mg/kg) was well below the maximum tolerated dose in mice. S phase arrest was also observed in tumors of bladder cancer patients receiving gemcitabine. The Chk1 inhibitor MK-8776 sensitized cells to gemcitabine with the greatest cell killing when added 18 h after gemcitabine. In mice, the administration of MK-8776 18 h after gemcitabine elicited positivity for the DNA damage marker γH2AX; this also occurred at relatively low dose (40 mg/kg) gemcitabine. Hence, in both cell culture and xenografts, MK-8776 can markedly enhance cell killing of cells reversibly arrested in S phase by gemcitabine. Some cell lines are hypersensitive to MK-8776 as monotherapy, but this was not observed in xenograft models. Effective monotherapy requires a higher dose of Chk1 inhibitor, and target inhibition over a longer time period as compared to its use in combination. These results have important implications for combining Chk1 inhibitors with gemcitabine and suggest that Chk1 inhibitors with increased bioavailability may have improved efficacy both in combination and as monotherapy.
吉西他滨不可逆地抑制核糖核苷酸还原酶并诱导S期阻滞,但这在小鼠肿瘤或患者肿瘤中是否发生尚未明确。将培养的肿瘤细胞与吉西他滨孵育6小时,以模拟患者的给药方案。此后诱导持续S期阻滞的浓度与细胞杀伤相关。给小鼠注射吉西他滨也显示其肿瘤中存在持续的S期阻滞。24小时后诱导几乎完全S期阻滞的最小剂量(40毫克/千克)远低于小鼠的最大耐受剂量。在接受吉西他滨治疗的膀胱癌患者的肿瘤中也观察到了S期阻滞。Chk1抑制剂MK-8776在吉西他滨给药18小时后添加时,使细胞对吉西他滨敏感,细胞杀伤作用最强。在小鼠中,吉西他滨给药18小时后注射MK-8776会使DNA损伤标志物γH2AX呈阳性;在相对低剂量(40毫克/千克)的吉西他滨时也会出现这种情况。因此,在细胞培养和异种移植中,MK-8776均可显著增强吉西他滨使处于S期可逆阻滞的细胞的杀伤作用。一些细胞系对MK-8776单药治疗高度敏感,但在异种移植模型中未观察到这种情况。有效的单药治疗需要更高剂量的Chk1抑制剂,且与联合使用相比,需要更长时间的靶点抑制。这些结果对于Chk1抑制剂与吉西他滨联合使用具有重要意义,并表明生物利用度增加的Chk1抑制剂在联合使用和单药治疗中可能具有更高的疗效。