Castel Amanda D, Terzian Arpi, Hart Rachel, Rayeed Nabil, Kalmin Mariah M, Young Heather, Greenberg Alan E
Department of Epidemiology and Biostatistics, Milken Institute School of Public Health, George Washington University, Washington, DC., United States of America.
Cerner Corporation, Kansas City, Missouri, United States of America.
PLoS One. 2017 Oct 5;12(10):e0186036. doi: 10.1371/journal.pone.0186036. eCollection 2017.
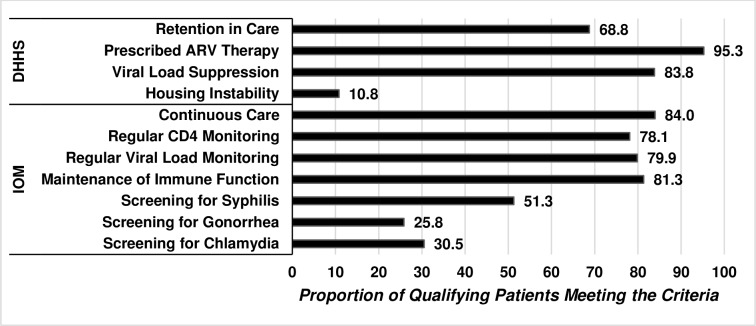
We sought to benchmark the quality of HIV care being received by persons living with HIV in care in Washington, DC and identify individual-level and structural-level differences. Data from the DC Cohort, an observational HIV cohort of persons receiving outpatient care in DC, were used to estimate the Institute of Medicine (IOM) and Department of Health and Human Services (HHS) quality of care measures. Differences in care by demographics and clinic type were assessed using χ2 tests and multivariable regression models. Among 8,047 participants, by HHS standards, 69% of participants were retained in care (RIC), 95% were prescribed antiretroviral therapy (ART), and 84% were virally suppressed (VS). By IOM standards, 84% were in continuous care; and 78% and 80% underwent regular CD4 and VL monitoring, respectively. Screening for syphilis, chlamydia, and gonorrhea was 51%, 31%, and 26%, respectively. Older participants were 1.5 times more likely to be RIC compared to younger participants (OR: 1.5; 95% CI: 1.3, 1.8). Participants enrolled in community-based clinics were more likely to be RIC (OR: 1.7; 95% CI: 1.4, 2.0) versus those enrolled at hospital-based clinics. Older participants were more likely to achieve VS than younger participants (OR: 1.8; 95% CI: 1.5, 2.2) while Black participants were less likely compared to white participants (OR: 0.4; 95% CI: 0.3, 0.5). Despite high measures of quality of care, disparities remain. Continued monitoring of the quality of HIV care and treatment can inform the development of public health programs and interventions to optimize care delivery.
我们试图评估华盛顿特区接受治疗的艾滋病毒感染者所接受的艾滋病毒护理质量,并确定个体层面和结构层面的差异。来自特区队列(一个在华盛顿特区接受门诊治疗的艾滋病毒观察性队列)的数据,被用于评估医学研究所(IOM)和卫生与公众服务部(HHS)的护理质量指标。使用卡方检验和多变量回归模型评估不同人口统计学特征和诊所类型在护理方面的差异。在8047名参与者中,按照HHS标准,69%的参与者接受了持续护理(RIC),95%的参与者接受了抗逆转录病毒疗法(ART),84%的参与者病毒得到抑制(VS)。按照IOM标准,84%的参与者接受了持续护理;分别有78%和80%的参与者接受了定期的CD4和病毒载量监测。梅毒、衣原体和淋病的筛查率分别为51%、31%和26%。与年轻参与者相比,老年参与者接受持续护理的可能性高1.5倍(比值比:1.5;95%置信区间:1.3,1.8)。与在医院诊所登记的参与者相比,在社区诊所登记的参与者更有可能接受持续护理(比值比:1.7;95%置信区间:1.4,2.0)。老年参与者比年轻参与者更有可能实现病毒抑制(比值比:1.8;95%置信区间:1.5,2.2),而黑人参与者与白人参与者相比可能性较小(比值比:0.4;95%置信区间:0.3,0.5)。尽管护理质量指标较高,但差异仍然存在。持续监测艾滋病毒护理和治疗质量可为制定公共卫生项目和干预措施提供信息,以优化护理服务。