Nguyen Thang, Le Khanh K, Cao Hoang T K, Tran Dao T T, Ho Linh M, Thai Trang N D, Pham Hoa T K, Pham Phong T, Nguyen Thao H, Hak Eelko, Pham Tam T, Taxis Katja
Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam.
Groningen Research Institute of Pharmacy, Unit of PharmacoTherapy, Epidemiology & Economics, University of Groningen, Groningen, The Netherlands.
BMJ Open. 2017 Oct 5;7(10):e017008. doi: 10.1136/bmjopen-2017-017008.
We aimed to determine the association between physician adherence to prescribing guideline-recommended medications during hospitalisation and 6-month major adverse outcomes of patients with acute coronary syndrome in Vietnam.
Prospective cohort study.
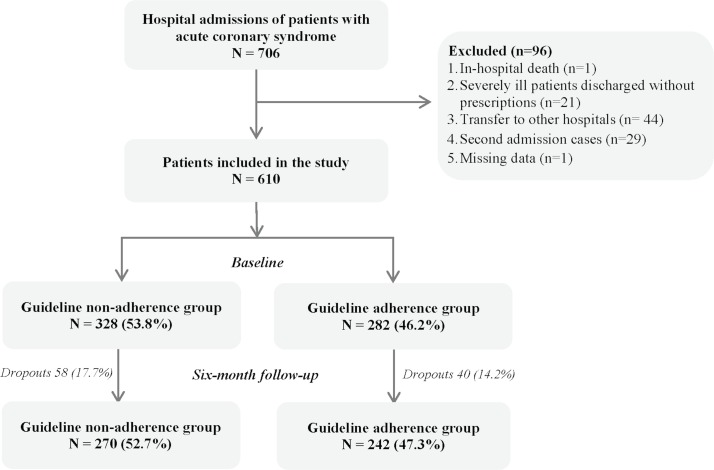
The study was carried out in two public hospitals in Vietnam between January and October 2015. Patients were followed for 6 months after discharge.
Patients who survived during hospitalisation with a discharge diagnosis of acute coronary syndrome and who were eligible for receiving at least one of the four guideline-recommended medications.
Guideline adherence was defined as prescribing all guideline-recommended medications at both hospital admission and discharge for eligible patients. Medications were antiplatelet agents, beta-blockers, ACE inhibitors or angiotensin II receptor blockers and statins.
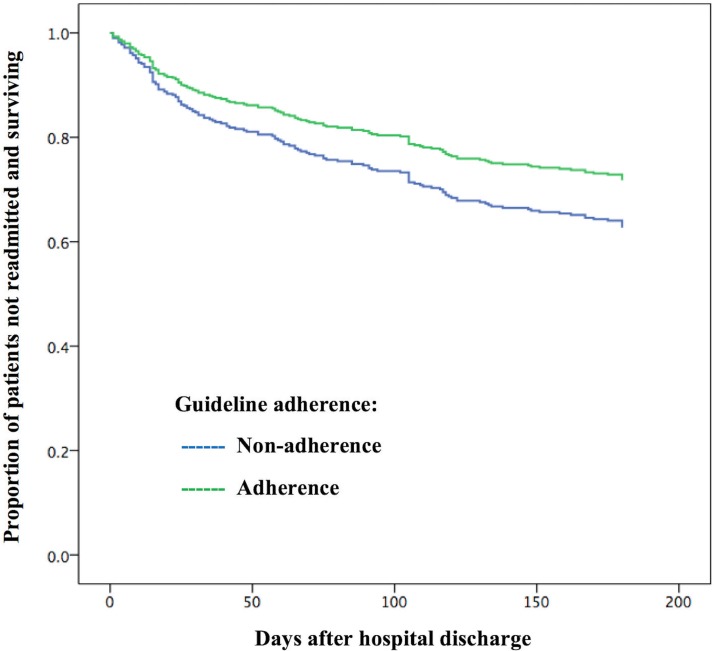
Six-month major adverse outcomes were defined as all-cause mortality or hospital readmission due to cardiovascular causes occurring during 6 months after discharge. Cox regression models were used to estimate the association between guideline adherence and 6-month major adverse outcomes.
Overall, 512 patients were included. Of those, there were 242 patients (47.3%) in the guideline adherence group and 270 patients (52.3%) in the non-adherence group. The rate of 6-month major adverse outcomes was 30.5%. A 29% reduction in major adverse outcomes at 6 months after discharge was found for patients of the guideline adherence group compared with the non-adherence group (adjusted HR, 0.71; 95% CI, 0.51 to 0.98; p=0.039). Covariates significantly associated with the major adverse outcomes were percutaneous coronary intervention, prior heart failure and renal insufficiency.
In-hospital guideline adherence was associated with a significant decrease in major adverse outcomes up to 6 months after discharge. It supports the need for improving adherence to guidelines in hospital practice in low-income and middle-income countries like Vietnam.
我们旨在确定越南急性冠脉综合征患者住院期间医生对处方指南推荐药物的依从性与6个月主要不良结局之间的关联。
前瞻性队列研究。
该研究于2015年1月至10月在越南的两家公立医院进行。患者出院后随访6个月。
住院期间存活且出院诊断为急性冠脉综合征、有资格接受四种指南推荐药物中至少一种的患者。
指南依从性定义为符合条件的患者在入院和出院时均开具所有指南推荐药物。药物包括抗血小板药物、β受体阻滞剂、血管紧张素转换酶抑制剂或血管紧张素II受体阻滞剂以及他汀类药物。
6个月主要不良结局定义为出院后6个月内发生的全因死亡率或因心血管原因再次入院。采用Cox回归模型估计指南依从性与6个月主要不良结局之间的关联。
总体纳入512例患者。其中,指南依从组有242例患者(47.3%),非依从组有270例患者(52.3%)。6个月主要不良结局发生率为30.5%。与非依从组相比,指南依从组患者出院后6个月主要不良结局降低了29%(校正风险比,0.71;95%置信区间,0.51至0.98;P = 0.039)。与主要不良结局显著相关的协变量为经皮冠状动脉介入治疗、既往心力衰竭和肾功能不全。
住院期间的指南依从性与出院后长达6个月的主要不良结局显著降低相关。这支持了在越南等低收入和中等收入国家的医院实践中提高对指南依从性的必要性。