Department of Radiation Oncology, Barrow Neurological Institute, St. Joseph's Hospital and Medical Center, Phoenix, Arizona.
NRG Oncology Statistics and Data Management Center, Philadelphia, Pennsylvania.
J Neurosurg. 2018 Jul;129(1):35-47. doi: 10.3171/2016.11.JNS161170. Epub 2017 Oct 6.
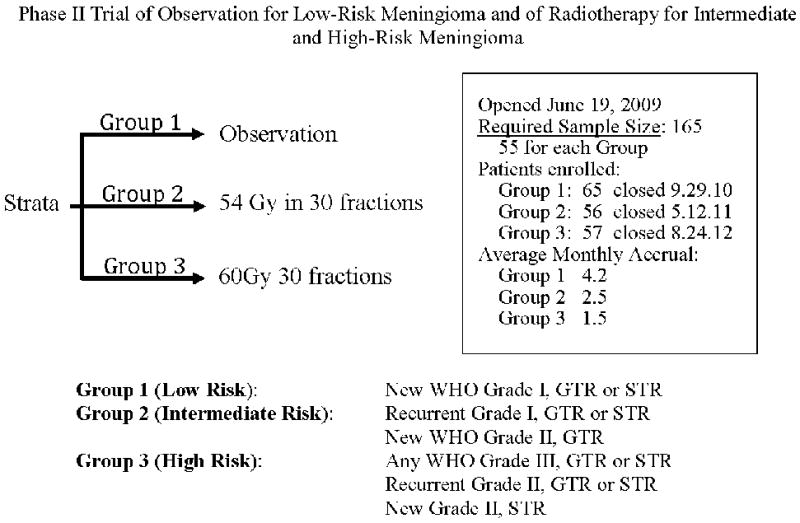
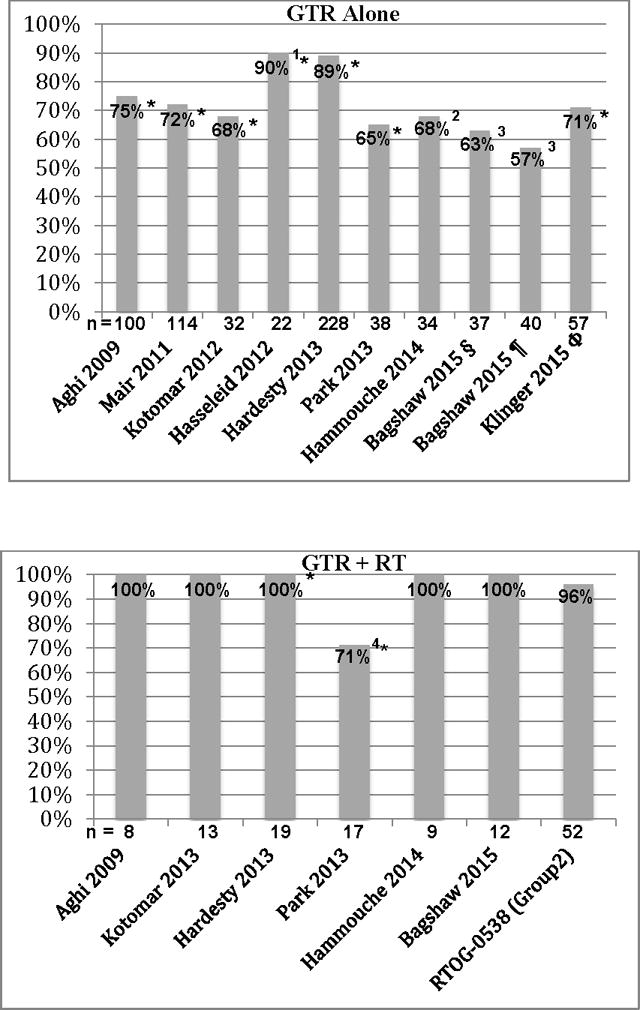
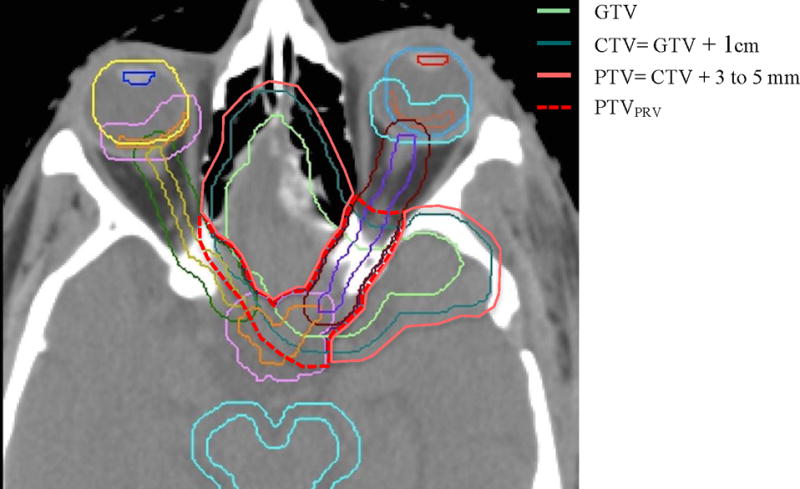
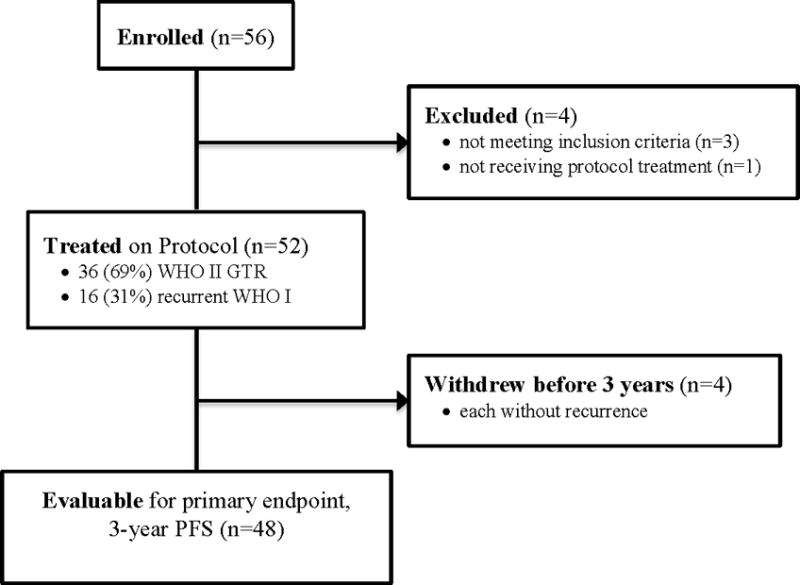
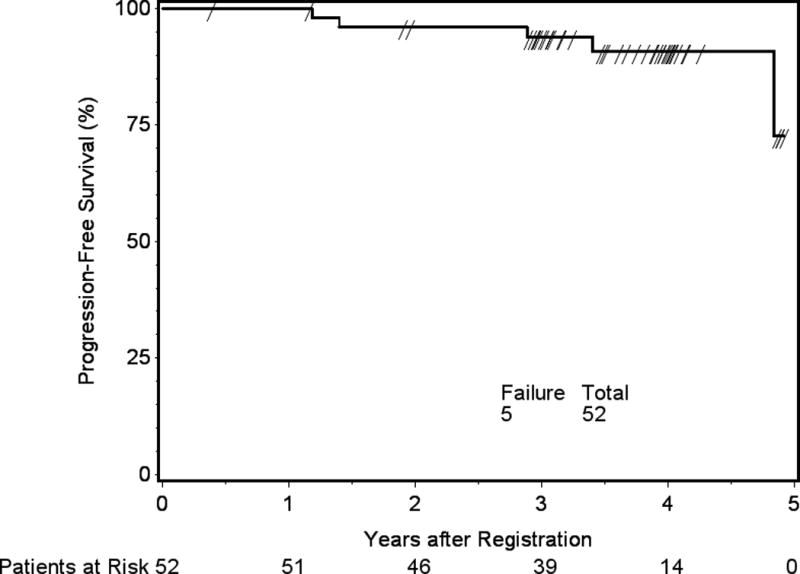
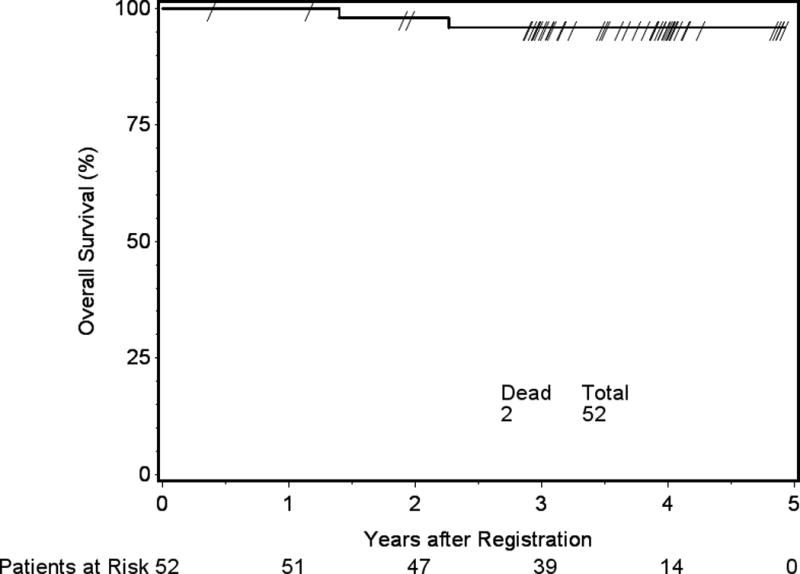
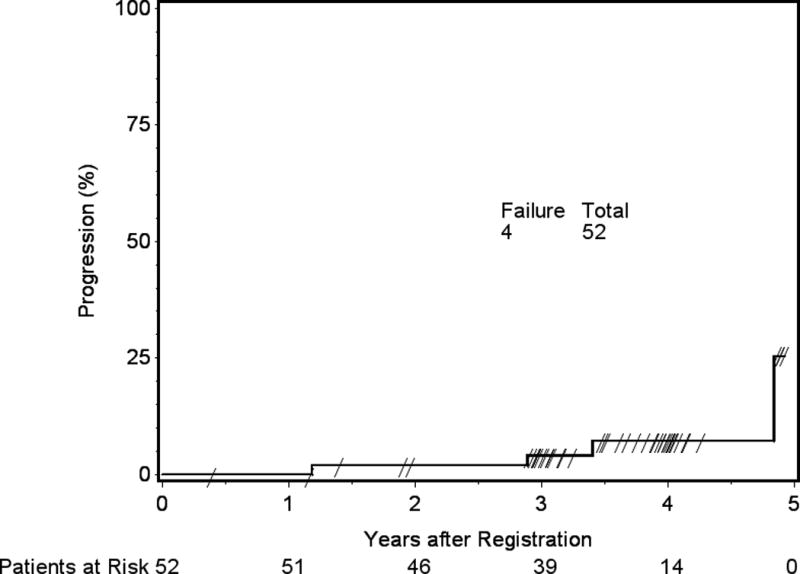
OBJECTIVE This is the first clinical outcomes report of NRG Oncology RTOG 0539, detailing the primary endpoint, 3-year progression-free survival (PFS), compared with a predefined historical control for intermediate-risk meningioma, and secondarily evaluating overall survival (OS), local failure, and prospectively scored adverse events (AEs). METHODS NRG Oncology RTOG 0539 was a Phase II clinical trial allocating meningioma patients to 1 of 3 prognostic groups and management strategies according to WHO grade, recurrence status, and resection extent. For the intermediate-risk group (Group 2), eligible patients had either newly diagnosed WHO Grade II meningioma that had been treated with gross-total resection (GTR; Simpson Grades I-III) or recurrent WHO Grade I meningioma with any resection extent. Pathology and imaging were centrally reviewed. Patients were treated with radiation therapy (RT), either intensity modulated (IMRT) or 3D conformal (3DCRT), 54 Gy in 30 fractions. The RT target volume was defined as the tumor bed and any nodular enhancement (e.g., in patients with recurrent WHO Grade I tumors) with a minimum 8-mm and maximum 15-mm margin, depending on tumor location and setup reproducibility of the RT method. The primary endpoint was 3-year PFS. Results were compared with historical controls (3-year PFS: 70% following GTR alone and 90% with GTR + RT). AEs were scored using NCI Common Toxicity Criteria. RESULTS Fifty-six patients enrolled in the intermediate-risk group, of whom 3 were ineligible and 1 did not receive RT. Of the 52 patients who received protocol therapy, 4 withdrew without a recurrence before 3 years leaving 48 patients evaluable for the primary endpoint, 3-year PFS, which was actuarially 93.8% (p = 0.0003). Within 3 years, 3 patients experienced events affecting PFS: 1 patient with a WHO Grade II tumor died of the disease, 1 patient with a WHO Grade II tumor had disease progression but remained alive, and 1 patient with recurrent WHO Grade I meningioma died of undetermined cause without tumor progression. The 3-year actuarial local failure rate was 4.1%, and the 3-year OS rate was 96%. After 3 years, progression occurred in 2 additional patients: 1 patient with recurrent WHO Grade I meningioma and 1 patient with WHO Grade II disease; both remain alive. Among 52 evaluable patients who received protocol treatment, 36 (69.2%) had WHO Grade II tumors and underwent GTR, and 16 (30.8%) had recurrent WHO Grade I tumors. There was no significant difference in PFS between these subgroups (p = 0.52, HR 0.56, 95% CI 0.09-3.35), validating their consolidation. Of the 52 evaluable patients, 44 (84.6%) received IMRT, and 50 (96.2%) were treated per protocol or with acceptable variation. AEs (definitely, probably, or possibly related to protocol treatment) were limited to Grade 1 or 2, with no reported Grade 3 events. CONCLUSIONS This is the first clinical outcomes report from NRG Oncology RTOG 0539. Patients with intermediate-risk meningioma treated with RT had excellent 3-year PFS, with a low rate of local failure and a low risk of AEs. These results support the use of postoperative RT for newly diagnosed gross-totally resected WHO Grade II or recurrent WHO Grade I meningioma irrespective of resection extent. They also document minimal toxicity and high rates of tumor control with IMRT. Clinical trial registration no.: NCT00895622 (clinicaltrials.gov).
这是 NRG 肿瘤学 RTOG 0539 的首次临床结果报告,详细介绍了主要终点,即与预先设定的中等风险脑膜瘤历史对照相比的 3 年无进展生存率(PFS),其次还评估了总生存率(OS)、局部失败率和前瞻性评分的不良事件(AE)。
NRG 肿瘤学 RTOG 0539 是一项 II 期临床试验,根据世界卫生组织(WHO)分级、复发情况和切除程度,将脑膜瘤患者分配到 3 个预后组和管理策略中。对于中等风险组(组 2),符合条件的患者要么是新诊断的 WHO 分级 II 型脑膜瘤,已经接受了大体全切除(GTR;Simpson 分级 I-III),要么是复发的 WHO 分级 I 型脑膜瘤,任何切除程度均可。病理学和影像学均进行了中心审查。患者接受放疗(RT),包括调强放疗(IMRT)或三维适形放疗(3DCRT),54 Gy 分 30 次。RT 靶区定义为肿瘤床和任何结节增强(例如,在复发的 WHO 分级 I 肿瘤患者中),最小 8mm,最大 15mm 边界,取决于肿瘤位置和 RT 方法的设置可重复性。主要终点是 3 年 PFS。结果与历史对照(单独 GTR 为 3 年 PFS:70%,GTR 加 RT 为 90%)进行比较。使用 NCI 常见毒性标准对 AE 进行评分。
56 例患者入组中等风险组,其中 3 例不符合条件,1 例未接受 RT。在接受方案治疗的 52 例患者中,4 例在 3 年内无复发前退出,48 例患者可评估主要终点,即 3 年 PFS,3 年 PFS的实际发生率为 93.8%(p = 0.0003)。在 3 年内,有 3 例患者发生影响 PFS 的事件:1 例 WHO 分级 II 肿瘤患者死于疾病,1 例 WHO 分级 II 肿瘤患者疾病进展但仍存活,1 例复发的 WHO 分级 I 脑膜瘤患者死于原因不明的无肿瘤进展。3 年局部失败率为 4.1%,3 年 OS 率为 96%。3 年后,又有 2 例患者进展:1 例复发的 WHO 分级 I 脑膜瘤患者,1 例 WHO 分级 II 疾病患者;均存活。在接受方案治疗的 52 例可评估患者中,36 例(69.2%)为 WHO 分级 II 肿瘤,接受 GTR,16 例(30.8%)为复发的 WHO 分级 I 肿瘤。这两个亚组之间的 PFS 无显著差异(p = 0.52,HR 0.56,95%CI 0.09-3.35),验证了它们的一致性。在 52 例可评估患者中,44 例(84.6%)接受了 IMRT,50 例(96.2%)按方案或可接受的变化进行了治疗。AE(肯定、可能或可能与方案治疗有关)限于 1 级或 2 级,无报告 3 级事件。
这是 NRG 肿瘤学 RTOG 0539 的首次临床结果报告。接受 RT 治疗的中等风险脑膜瘤患者 3 年 PFS 优异,局部失败率低,AE 风险低。这些结果支持对新诊断的 WHO 分级 II 型或复发的 WHO 分级 I 型脑膜瘤进行术后 RT,无论切除程度如何。它们还记录了 IMRT 的最小毒性和高肿瘤控制率。临床试验注册号:NCT00895622(clinicaltrials.gov)。