Eckert Erin, Florey Lia S, Tongren Jon Eric, Salgado S René, Rukundo Alphonse, Habimana Jean Pierre, Hakizimana Emmanuel, Munguti Kaendi, Umulisa Noella, Mulindahabi Monique, Karema Corine
President's Malaria Initiative (PMI), U.S. Agency for International Development (USAID), Washington, District of Columbia.
ICF, Rockville, Maryland.
Am J Trop Med Hyg. 2017 Sep;97(3_Suppl):99-110. doi: 10.4269/ajtmh.17-0281.
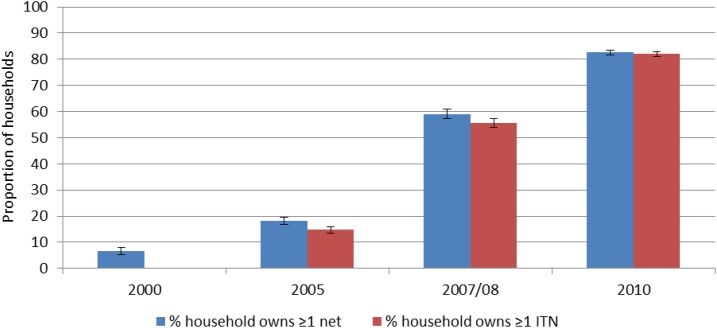
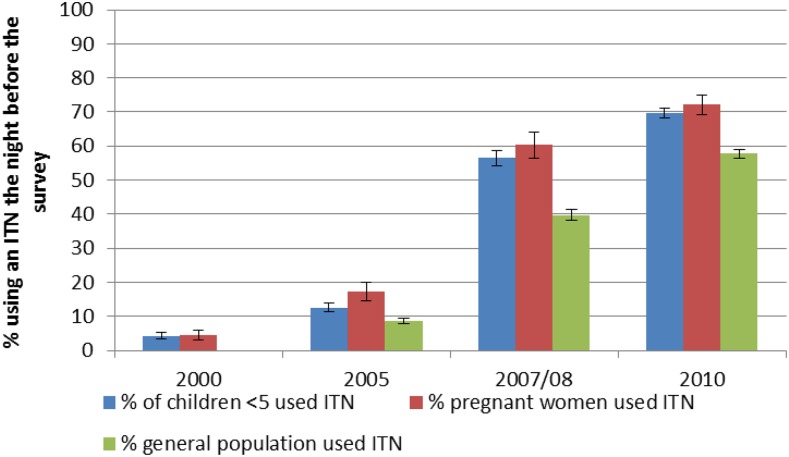
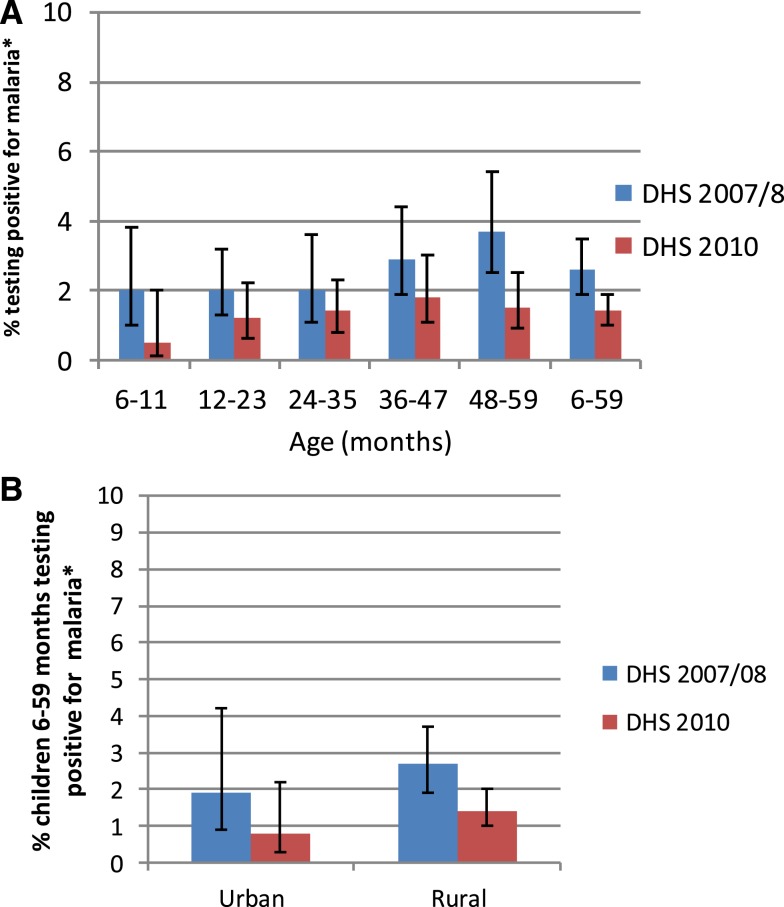
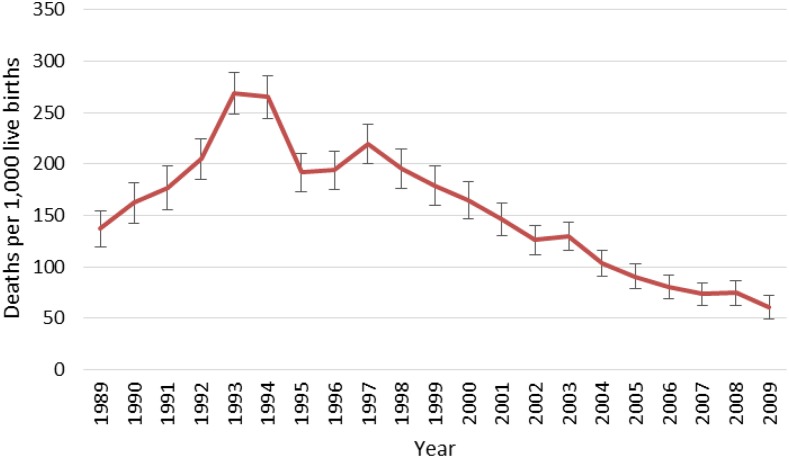
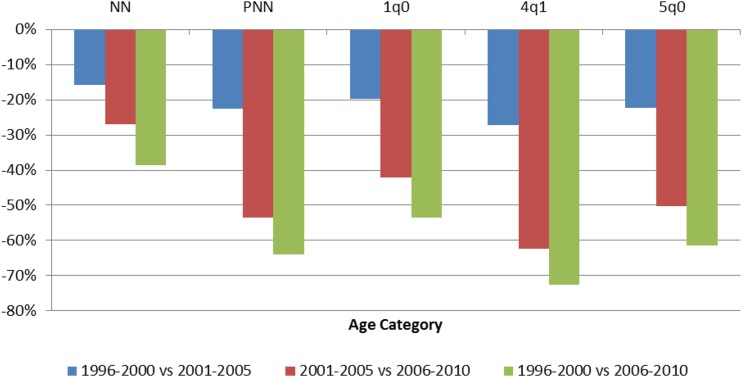
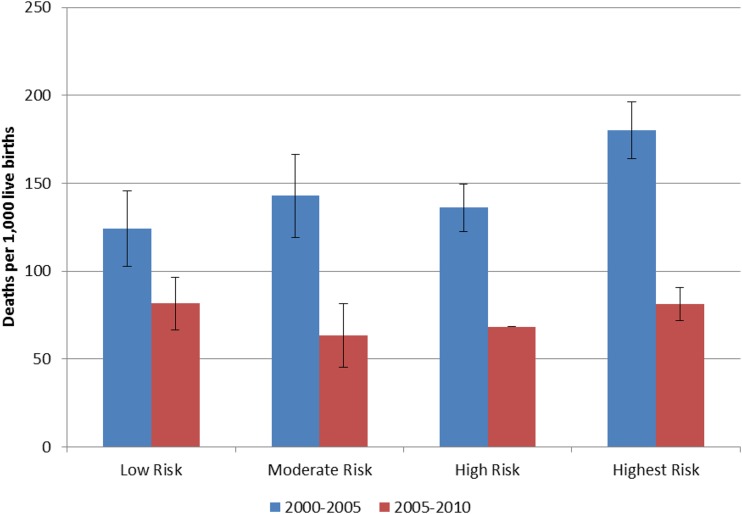
The impressive decline in child mortality that occurred in Rwanda from 1996-2000 to 2006-2010 coincided with a period of rapid increase of malaria control interventions such as indoor residual spraying (IRS); insecticide-treated net (ITN) distribution and use, and improved malaria case management. The impact of these interventions was examined through ecological correlation analysis, and robust decomposition analysis of contextual factors on all-cause child mortality. Child mortality fell 61% during the evaluation period and prevalence of severe anemia in children 6-23 months declined 71% between 2005 and 2010. These changes in malaria morbidity and mortality occurred concurrently with a substantial increase in vector control activities. ITN use increased among children under five, from 4% to 70%. The IRS program began in 2007 and covered 1.3 million people in the highest burden districts by 2010. At the same time, diagnosis and treatment with an effective antimalarial expanded nationally, and included making services available to children under the age of 5 at the community level. The percentage of children under 5 who sought care for a fever increased from 26% in 2000 to 48% in 2010. Multivariable models of the change in child mortality between 2000 and 2010 using nationally representative data reveal the importance of increasing ITN ownership in explaining the observed mortality declines. Taken as a whole, the evidence supports the conclusion that malaria control interventions contributed to the observed decline in child mortality in Rwanda from 2000 to 2010, even in a context of improving socioeconomic, maternal, and child health conditions.
1996 - 2000年至2006 - 2010年期间,卢旺达儿童死亡率显著下降,这一时期恰逢疟疾控制干预措施迅速增加,如室内滞留喷洒(IRS);经杀虫剂处理蚊帐(ITN)的分发和使用,以及疟疾病例管理的改善。通过生态相关性分析以及对全因儿童死亡率的背景因素进行稳健分解分析,考察了这些干预措施的影响。在评估期间,儿童死亡率下降了61%,2005年至2010年期间,6 - 23个月儿童的重度贫血患病率下降了71%。疟疾发病率和死亡率的这些变化与病媒控制活动的大幅增加同时发生。五岁以下儿童的ITN使用率从4%增至70%。IRS项目于2007年启动,到2010年已覆盖负担最重地区的130万人。与此同时,有效的抗疟药物的诊断和治疗在全国范围内得到推广,包括在社区层面为五岁以下儿童提供服务。因发烧就医的五岁以下儿童比例从2000年的26%增至2010年的48%。利用全国代表性数据建立的2000年至2010年儿童死亡率变化多变量模型显示,增加ITN拥有量对于解释观察到的死亡率下降具有重要意义。总体而言,有证据支持这样的结论:即使在社会经济、孕产妇和儿童健康状况不断改善的背景下,疟疾控制干预措施仍有助于卢旺达2000年至2010年观察到的儿童死亡率下降。