Hershey Christine L, Florey Lia S, Ali Doreen, Bennett Adam, Luhanga Misheck, Mathanga Don P, Salgado S René, Nielsen Carrie F, Troell Peter, Jenda Gomezgani, Yé Yazoume, Bhattarai Achuyt
President's Malaria Initiative, Agency for International Development, Washington, District of Columbia.
The DHS Program, ICF International, Rockville, Maryland.
Am J Trop Med Hyg. 2017 Sep;97(3_Suppl):76-88. doi: 10.4269/ajtmh.17-0203.
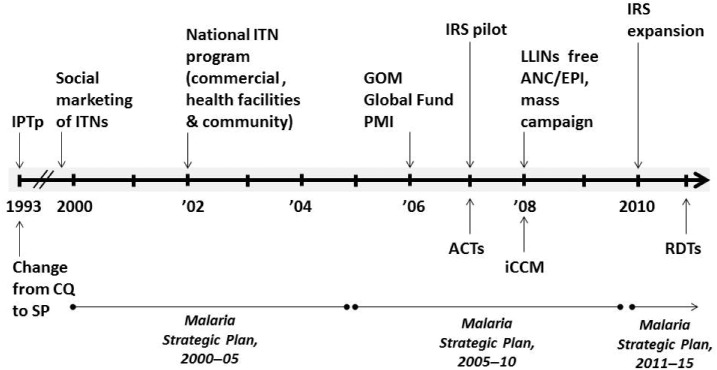
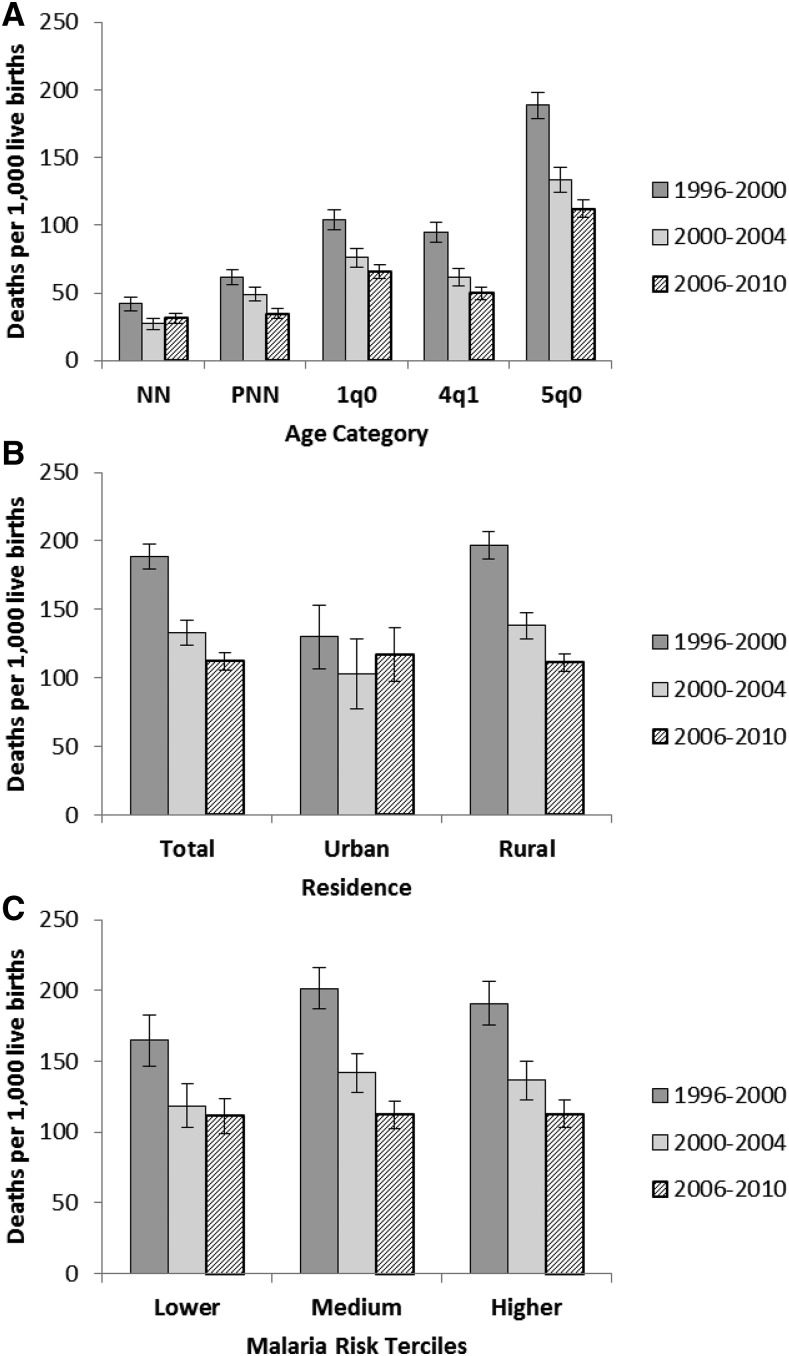
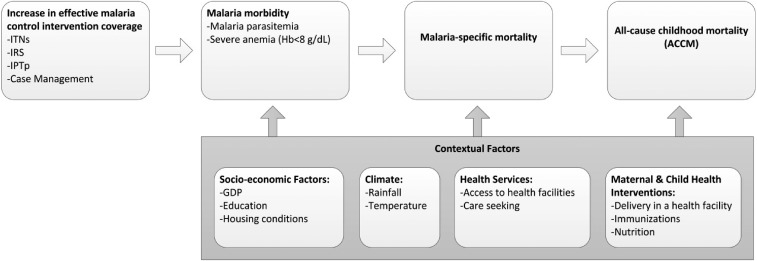
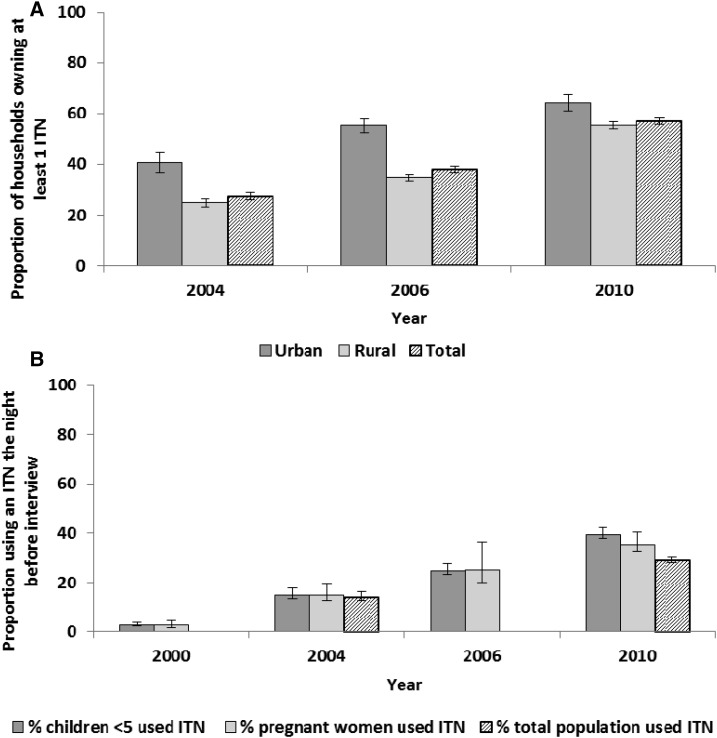
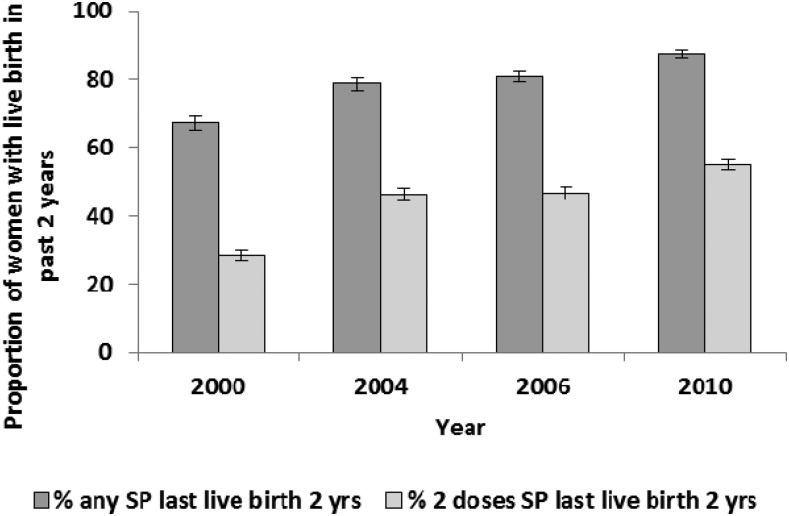
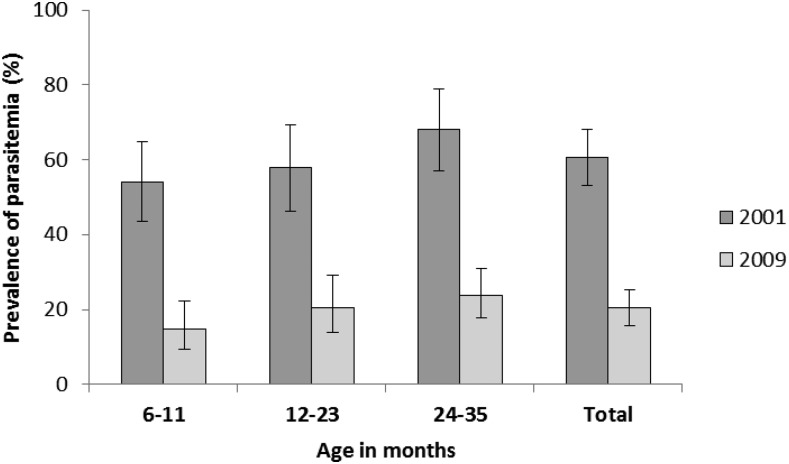
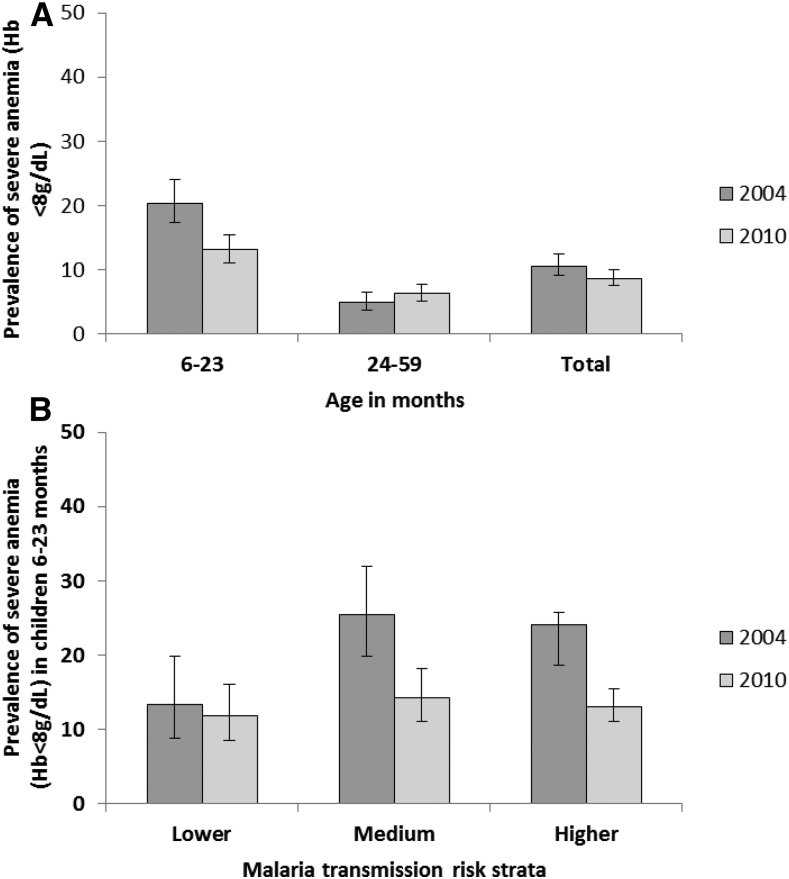
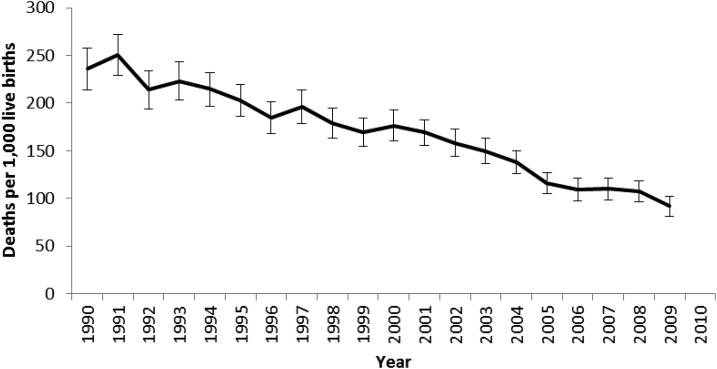
Malaria control intervention coverage increased nationwide in Malawi during 2000-2010. Trends in intervention coverage were assessed against trends in malaria parasite prevalence, severe anemia (hemoglobin < 8 g/dL), and all-cause mortality in children under 5 years of age (ACCM) using nationally representative household surveys. Associations between insecticide-treated net (ITN) ownership, malaria morbidity, and ACCM were also assessed. Household ITN ownership increased from 27.4% (95% confidence interval [CI] = 25.9-29.0) in 2004 to 56.8% (95% CI = 55.6-58.1) in 2010. Similarly intermittent preventive treatment during pregnancy coverage increased from 28.2% (95% CI = 26.7-29.8) in 2000 to 55.0% (95% CI = 53.4-56.6) in 2010. Malaria parasite prevalence decreased significantly from 60.5% (95% CI = 53.0-68.0) in 2001 to 20.4% (95% CI = 15.7-25.1) in 2009 in children aged 6-35 months. Severe anemia prevalence decreased from 20.4% (95% CI: 17.3-24.0) in 2004 to 13.1% (95% CI = 11.0-15.4) in 2010 in children aged 6-23 months. ACCM decreased 41%, from 188.6 deaths per 1,000 live births (95% CI = 179.1-198.0) during 1996-2000, to 112.1 deaths per 1,000 live births (95% CI = 105.8-118.5) during 2006-2010. When controlling for other covariates in random effects logistic regression models, household ITN ownership was protective against malaria parasitemia in children (odds ratio [OR] = 0.81, 95% CI = 0.72-0.92) and severe anemia (OR = 0.82, 95% CI = 0.72-0.94). After considering the magnitude of changes in malaria intervention coverage and nonmalaria factors, and given the contribution of malaria to all-cause mortality in malaria-endemic countries, the substantial increase in malaria control interventions likely improved child survival in Malawi during 2000-2010.
2000 - 2010年期间,马拉维全国疟疾控制干预措施的覆盖率有所提高。利用具有全国代表性的家庭调查,根据疟疾寄生虫感染率、重度贫血(血红蛋白<8 g/dL)以及5岁以下儿童全死因死亡率(ACCM)的趋势,评估了干预措施覆盖率的变化趋势。还评估了经杀虫剂处理蚊帐(ITN)的拥有情况、疟疾发病率与ACCM之间的关联。家庭ITN拥有率从2004年的27.4%(95%置信区间[CI]=25.9 - 29.0)增至2010年的56.8%(95% CI = 55.6 - 58.1)。同样,孕期间歇性预防治疗的覆盖率从2000年的28.2%(95% CI = 26.7 - 29.8)增至2010年的55.0%(95% CI = 53.4 - 56.6)。6 - 35个月龄儿童的疟疾寄生虫感染率从2001年的60.5%(95% CI = 53.0 - 68.0)显著降至2009年的20.4%(95% CI = 15.7 - 25.1)。6 - 23个月龄儿童的重度贫血患病率从2004年的20.4%(95% CI:17.3 - 24.0)降至2010年的13.1%(95% CI = 11.0 - 15.4)。ACCM下降了41%,从1996 - 2000年期间每1000例活产188.6例死亡(95% CI = 179.1 - 198.0)降至2006 - 2010年期间每1000例活产112.1例死亡(95% CI = 105.8 - 118.5)。在随机效应逻辑回归模型中对其他协变量进行控制后,家庭ITN拥有情况对儿童疟疾寄生虫血症具有保护作用(比值比[OR]=0.81,95% CI = 0.72 - 0.92)以及对重度贫血具有保护作用(OR = 0.82,95% CI = 0.72 - 0.94)。在考虑了疟疾干预措施覆盖率和非疟疾因素变化的幅度,并鉴于疟疾对疟疾流行国家全死因死亡率的影响后,2000 - 2010年期间疟疾控制干预措施的大幅增加可能改善了马拉维儿童的生存状况。