Collins Deirdre A, Hoskins Anke, Snelling Thomas, Senasinghe Kalpani, Bowman Jacinta, Stemberger Natalie A, Leach Amanda J, Lehmann Deborah
School of Medical and Health Sciences, Edith Cowan University, Perth, WA Australia.
Wesfarmers Centre of Vaccines & Infectious Diseases, Telethon Kids Institute, University of Western Australia, Perth, WA Australia.
Pneumonia (Nathan). 2017 Sep 25;9:14. doi: 10.1186/s41479-017-0038-x. eCollection 2017.
The 7-valent pneumococcal conjugate vaccine (PCV7) was introduced to prevent invasive pneumococcal disease (IPD) in Western Australian (WA) Aboriginal people in 2001. PCV13 replaced PCV7 in July 2011, covering six additional pneumococcal serotypes; however, IPD rates remained high in Aboriginal people in WA. Upper respiratory tract pneumococcal carriage can precede IPD, and PCVs alter serotype distribution.
To assess the impact of PCV13 introduction, identify emerging serotypes, and assess risk factors for carriage, nasopharyngeal swabs and information on demographic characteristics, health, medication and living conditions from Aboriginal children and adults across WA from August 2008 to November 2014 were collected. Bacteria were cultured using selective media and pneumococcal isolates were serotyped by Quellung reaction. Risk factors were analysed by multivariable logistic regression.
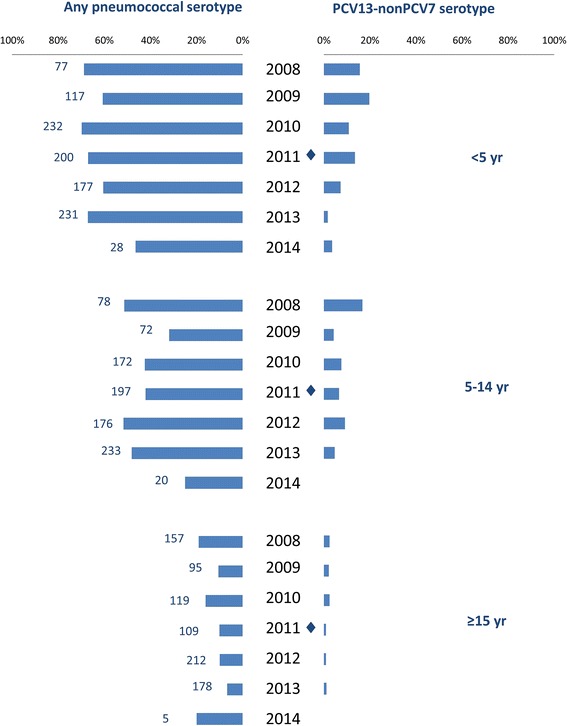
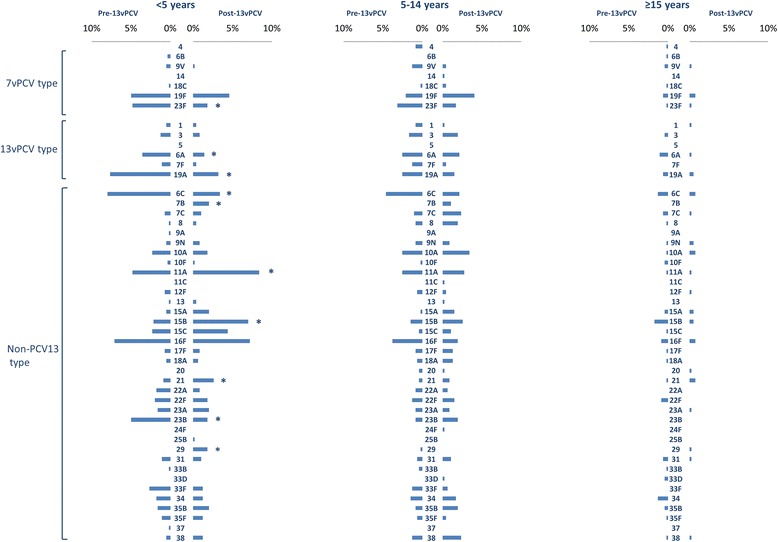
One thousand five hundred swabs pre- and 1385 swabs post-PCV13 introduction were collected. Pneumococcal carriage was detected in 66.8% of children <5 years old and 53.2% of 5-14 year-olds post-PCV13, compared with pre-PCV13 prevalence of 72.2% and 49.4%, respectively. The prevalence of PCV13-non-PCV7 serotypes decreased in children <5 years old from 13.5% pre-PCV13 to 5.8% post-PCV13 ( < 0.01), and from 8.4% to 6.1% in children 5-14 years old ( > 0.05). The most common serotypes post-PCV13 were 11A (prevalence 4.0%), 15B (3.5%), 16F (3.5%), and 19F (3.2%). Risk of detection of pneumococcal carriage increased until age 12 months (odds ratio [OR] 4.19, 95% confidence interval [CI] 2.39-7.33), with nasal discharge (OR 2.49 [95% CI 2.00-3.09]), residence in a remote community (OR 2.21 [95% CI 1.67-2.92]) and household crowding (OR 1.36 [95% CI 1.11-1.67]). Recent antibiotic use was negatively associated with pneumococcal carriage (OR 0.48 [95% CI 0.33-0.69]). Complete resistance to penicillin was present among isolates of serotypes 19A (6.0%), 19F (2.3%) and non-serotypeable isolates (1.9%). Serotype 23F and newly emerged serotype 7B isolates showed high rates of resistance to cotrimoxazole, erythromycin and tetracycline (86.9%, 86.9%, 82.0%, respectively for 23F, 100.0%, 100.0% and 93.3% for 7B).
Since PCV13 replaced PCV7, carriage of PCV13-non-PCV7 serotypes decreased significantly among children <5 years old, those most likely to have received PCV13, and to a lesser extent in older people. Known risk factors for carriage including crowding and young age remain in the Aboriginal population.
2001年,7价肺炎球菌结合疫苗(PCV7)被引入西澳大利亚州(WA)的原住民中,以预防侵袭性肺炎球菌疾病(IPD)。2011年7月,PCV13取代了PCV7,覆盖了另外6种肺炎球菌血清型;然而,WA原住民中的IPD发病率仍然很高。上呼吸道肺炎球菌携带可能先于IPD出现,并且PCV会改变血清型分布。
为评估引入PCV13的影响、识别新出现的血清型并评估携带的危险因素,收集了2008年8月至2014年11月期间WA各地原住民儿童和成人的鼻咽拭子以及有关人口统计学特征、健康状况、用药情况和生活条件的信息。使用选择性培养基培养细菌,并通过荚膜肿胀反应对肺炎球菌分离株进行血清分型。通过多变量逻辑回归分析危险因素。
在引入PCV13之前收集了1500份拭子,之后收集了1385份拭子。PCV13引入后,5岁以下儿童中肺炎球菌携带率为66.8%,5至14岁儿童中为53.2%,而PCV13引入前的患病率分别为72.2%和49.4%。5岁以下儿童中PCV13非PCV7血清型的患病率从PCV13引入前的13.5%降至引入后的5.8%(<0.01),5至14岁儿童中从8.4%降至6.1%(>0.05)。PCV13引入后最常见的血清型为11A(患病率4.0%)、15B(3.5%)、16F(3.5%)和19F(3.2%)。肺炎球菌携带的检出风险在12个月龄前增加(优势比[OR]4.19,95%置信区间[CI]2.39 - 7.33),伴有流涕(OR 2.49[95%CI 2.00 - 3.09])、居住在偏远社区(OR 2.21[95%CI 1.67 - 2.92])和家庭拥挤(OR 1.36[95%CI 1.11 - 1.67])。近期使用抗生素与肺炎球菌携带呈负相关(OR 0.48[95%CI 0.33 - 0.69])。19A血清型(6.0%)、19F血清型(2.3%)和不可分型分离株(1.9%)的分离株对青霉素完全耐药。23F血清型和新出现的7B血清型分离株对复方新诺明、红霉素和四环素显示出高耐药率(23F分别为86.9%、86.9%、82.0%,7B分别为100.0%、100.0%和93.3%)。
自从PCV13取代PCV-7以来,在最有可能接种PCV13的5岁以下儿童中,PCV13非PCV7血清型的携带率显著下降,在年龄较大人群中下降幅度较小。原住民人群中已知的携带危险因素,包括拥挤和低龄,仍然存在。