Chen Feng, Duan Guangyou, Wu Zhuoxi, Zuo Zhiyi, Li Hong
Department of Anesthesiology, Xinqiao Hospital, Third Military Medical University, Chongqing, China.
Department of Anesthesiology, University of Virginia, Charlottesville, Virginia, USA.
BMJ Open. 2017 Oct 11;7(10):e014629. doi: 10.1136/bmjopen-2016-014629.
Neurological dysfunction remains a devastating postoperative complication in patients undergoing cardiac surgery with cardiopulmonary bypass (CPB), and previous studies have shown that inhalation anaesthesia and total intravenous anaesthesia (TIVA) may produce different degrees of cerebral protection in these patients. Therefore, we conducted a systematic literature review and meta-analysis to compare the neuroprotective effects of inhalation anaesthesia and TIVA.
Searching in PubMed, EMBASE, Science Direct/Elsevier, China National Knowledge Infrastructure and Cochrane Library up to August 2016, we selected related randomised controlled trials for this meta-analysis.
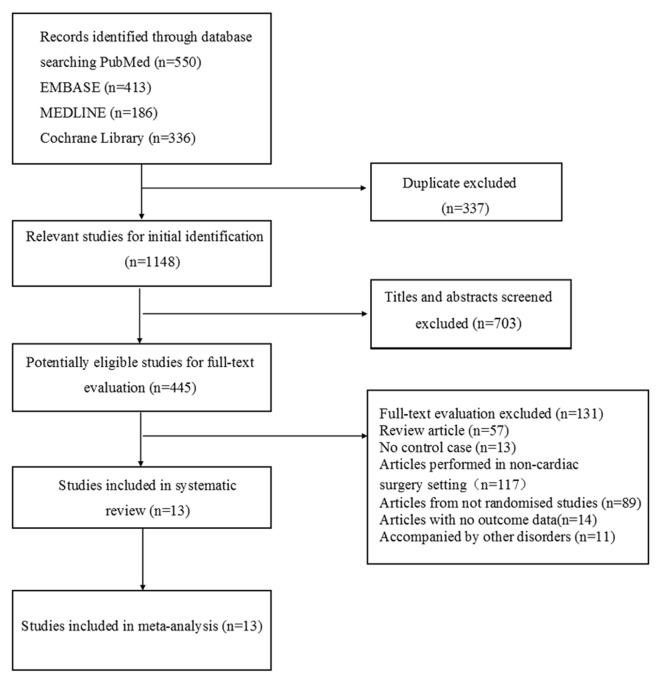
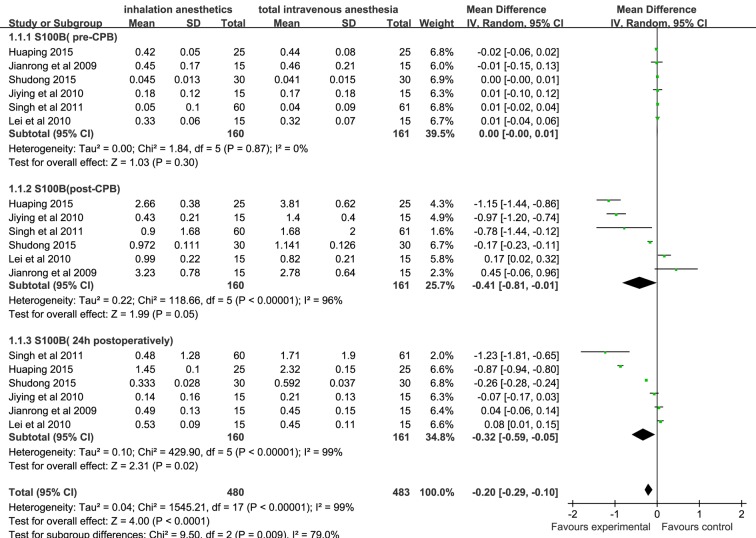
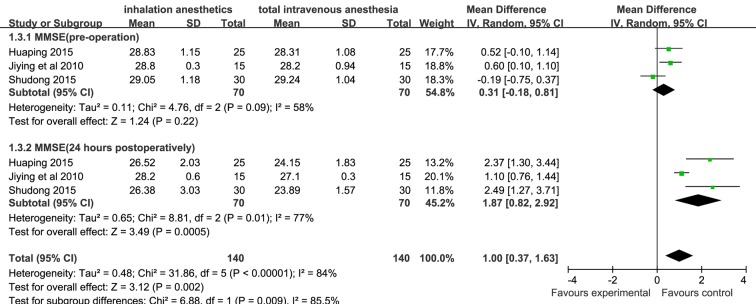
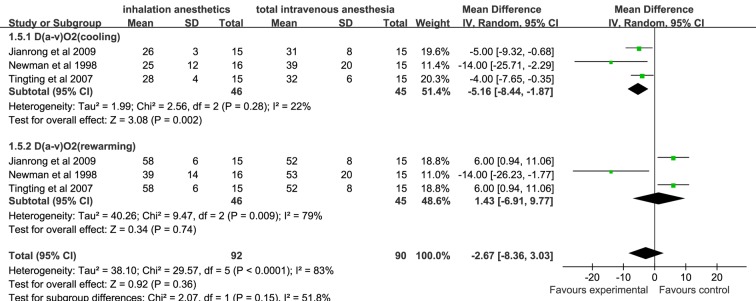
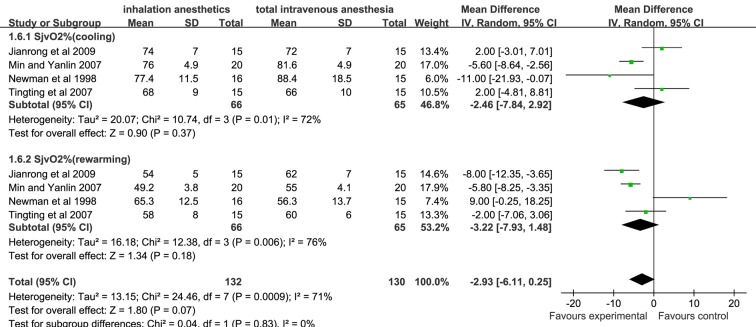
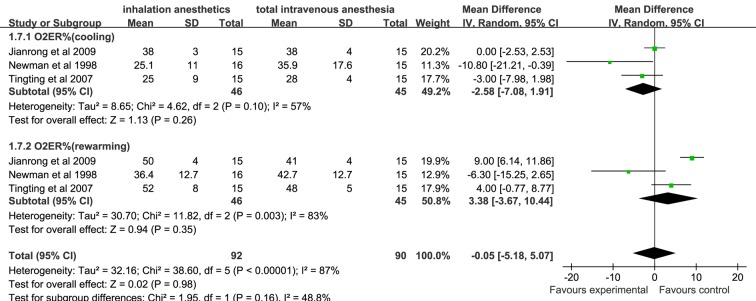
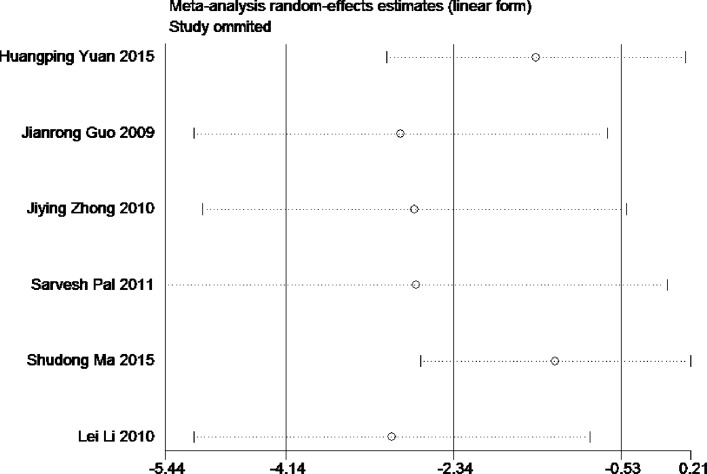
A total of 1485 studies were identified. After eliminating duplicate articles and screening titles and abstracts, 445 studies were potentially eligible. After applying exclusion criteria (full texts reported as abstracts, review article, no control case, lack of outcome data and so on), 13 studies were selected for review. Our results demonstrated that the primary outcome related to S100B level in the inhalation anaesthesia group was significantly lower than in the TIVA group after CPB and 24 hours postoperatively (weighted mean difference (WMD); 95% CI (CI): -0.41(-0.81 to -0.01), -0.32 (-0.59 to -0.05), respectively). Among secondary outcome variables, mini-mental state examination scores of the inhalation anaesthesia group were significantly higher than those of the TIVA group 24 hours after operation (WMD (95% CI): 1.87 (0.82 to 2.92)), but no significant difference was found in arteriovenous oxygen content difference, cerebral oxygen extraction ratio and jugular bulb venous oxygen saturation, which were assessed at cooling and rewarming during CPB.
This study demonstrates that anaesthesia with volatile agents appears to provide better cerebral protection than TIVA for patients undergoing cardiac surgery with CPB, suggesting that inhalation anaesthesia may be more suitable for patients undergoing cardiac surgery.
神经功能障碍仍是接受体外循环(CPB)心脏手术患者术后的一种毁灭性并发症,既往研究表明,吸入麻醉和全静脉麻醉(TIVA)在这些患者中可能产生不同程度的脑保护作用。因此,我们进行了一项系统的文献综述和荟萃分析,以比较吸入麻醉和TIVA的神经保护作用。
截至2016年8月,在PubMed、EMBASE、Science Direct/Elsevier、中国知网和Cochrane图书馆中进行检索,我们选择相关随机对照试验进行这项荟萃分析。
共识别出1485项研究。在剔除重复文章并筛选标题和摘要后,445项研究可能符合条件。应用排除标准(全文报道为摘要、综述文章、无对照病例、缺乏结局数据等)后,选择13项研究进行综述。我们的结果表明,CPB后及术后24小时,吸入麻醉组与S100B水平相关的主要结局显著低于TIVA组(加权平均差(WMD);95%可信区间(CI):分别为-0.41(-0.81至-0.01),-0.32(-0.59至-0.05))。在次要结局变量中,吸入麻醉组术后24小时的简易精神状态检查评分显著高于TIVA组(WMD(95%CI):1.87(0.8至2.92)),但在CPB期间降温及复温时评估的动静脉氧含量差、脑氧摄取率和颈静脉球部血氧饱和度方面未发现显著差异。
本研究表明,对于接受CPB心脏手术的患者,挥发性药物麻醉似乎比TIVA提供更好的脑保护,提示吸入麻醉可能更适合接受心脏手术的患者。