Mossa-Basha Mahmud, Shibata Dean K, Hallam Danial K, de Havenon Adam, Hippe Daniel S, Becker Kyra J, Tirschwell David L, Hatsukami Thomas, Balu Niranjan, Yuan Chun
From the Department of Radiology (M.M.-B., D.K.S., D.K.H., D.S.H., N.B., C.Y.), Department of Neurology (K.J.B., D.L.T.), and Department of Surgery (T.H.), University of Washington, Seattle; and Department of Neurology, University of Utah, Salt Lake City (A.D.H.).
Stroke. 2017 Nov;48(11):3026-3033. doi: 10.1161/STROKEAHA.117.018227. Epub 2017 Oct 13.
Our goal is to determine the added value of intracranial vessel wall magnetic resonance imaging (IVWI) in differentiating nonocclusive vasculopathies compared with luminal imaging alone.
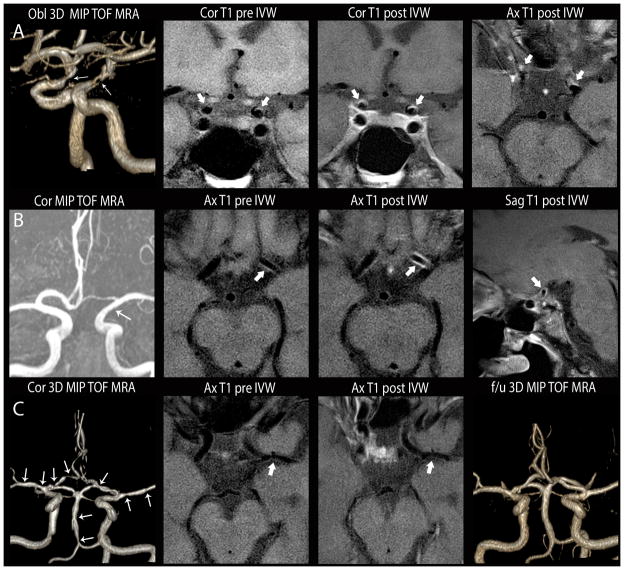
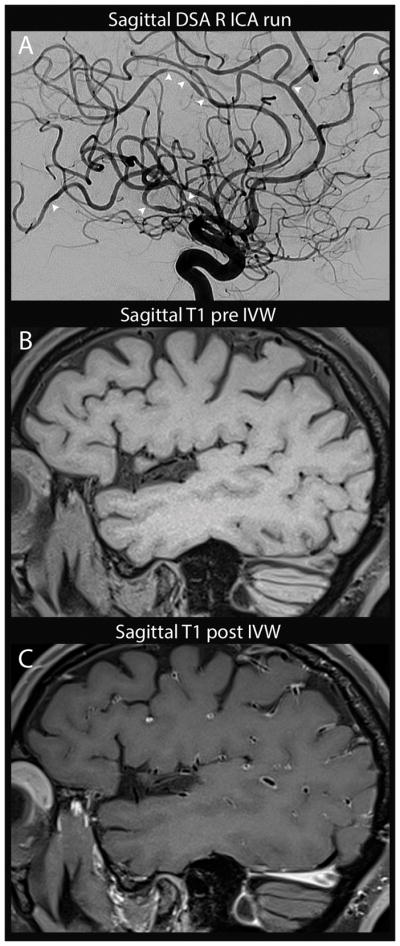
We retrospectively reviewed images from patients with both luminal and IVWI to identify cases with clinically defined intracranial vasculopathies: atherosclerosis (intracranial atherosclerotic disease), reversible cerebral vasoconstriction syndrome, and inflammatory vasculopathy. Two neuroradiologists blinded to clinical data reviewed the luminal imaging of defined luminal stenoses/irregularities and evaluated the pattern of involvement to make a presumed diagnosis with diagnostic confidence. Six weeks later, the 2 raters rereviewed the luminal imaging in addition to IVWI for the pattern of wall involvement, presence and pattern of postcontrast enhancement, and presumed diagnosis and confidence. Analysis was performed on per-lesion and per-patient bases.
Thirty intracranial atherosclerotic disease, 12 inflammatory vasculopathies, and 12 reversible cerebral vasoconstriction syndrome patients with 201 lesions (90 intracranial atherosclerotic disease, 64 reversible cerebral vasoconstriction syndrome, and 47 inflammatory vasculopathy lesions) were included. For both per-lesion and per-patient analyses, there was significant diagnostic accuracy improvement with luminal imaging+IVWI when compared with luminal imaging alone (per-lesion: 88.8% versus 36.1%; <0.001 and per-patient: 96.3% versus 43.5%; <0.001, respectively). There was substantial interrater diagnostic agreement for luminal imaging+IVWI (κ=0.72) and only slight agreement for luminal imaging (κ=0.04). Although there was a significant correlation for both luminal and IVWI pattern of wall involvement with diagnosis, there was a stronger correlation for IVWI finding of lesion eccentricity and intracranial atherosclerotic disease diagnosis than for luminal imaging (κ=0.69 versus 0.18; <0.001).
IVWI can significantly improve the differentiation of nonocclusive intracranial vasculopathies when combined with traditional luminal imaging modalities.
我们的目标是确定颅内血管壁磁共振成像(IVWI)与单纯管腔成像相比,在鉴别非闭塞性血管病变方面的附加价值。
我们回顾性分析了同时接受管腔成像和IVWI检查的患者图像,以确定临床诊断为颅内血管病变的病例:动脉粥样硬化(颅内动脉粥样硬化疾病)、可逆性脑血管收缩综合征和炎症性血管病变。两位对临床数据不知情的神经放射科医生对已确定管腔狭窄/不规则的管腔成像进行了回顾,并评估了受累模式,以做出具有诊断信心的推测性诊断。六周后,这两位评估者除了对IVWI进行回顾外,还重新回顾了管腔成像,以观察血管壁受累模式、增强后强化的存在及模式、推测性诊断和信心。分析是基于每个病变和每个患者进行的。
纳入了30例颅内动脉粥样硬化疾病、12例炎症性血管病变和12例可逆性脑血管收缩综合征患者,共201个病变(90个颅内动脉粥样硬化疾病病变、64个可逆性脑血管收缩综合征病变和47个炎症性血管病变)。对于每个病变和每个患者的分析,与单纯管腔成像相比,管腔成像+IVWI的诊断准确性均有显著提高(每个病变:88.8%对36.1%;<0.001,每个患者:96.3%对43.5%;<0.001)。管腔成像+IVWI的评估者间诊断一致性较高(κ=0.72),而管腔成像的一致性仅为轻微(κ=0.04)。虽然管腔和IVWI的血管壁受累模式与诊断均存在显著相关性,但IVWI发现病变偏心性与颅内动脉粥样硬化疾病诊断的相关性比管腔成像更强(κ=0.69对0.18;<0.001)。
IVWI与传统管腔成像方式联合使用时,可显著提高对非闭塞性颅内血管病变的鉴别能力。