Inambao Mubiana, Kilembe William, Canary Lauren A, Czaicki Nancy L, Kakungu-Simpungwe Matilda, Chavuma Roy, Wall Kristin M, Tichacek Amanda, Pulerwitz Julie, Thior Ibou, Chomba Elwyn, Allen Susan A
Rwanda Zambia HIV Research Group, Department of Pathology & Laboratory Medicine, School of Medicine and Hubert Department of Global Health, Rollins School of Public Health, Emory University, Atlanta, GA, United States of America.
Zambia Emory HIV Research Project (ZEHRP), Ndola, Zambia.
PLoS One. 2017 Oct 16;12(10):e0185142. doi: 10.1371/journal.pone.0185142. eCollection 2017.
Most HIV infections in Africa are acquired by married/cohabiting adults and WHO recommends couple's voluntary HIV counseling and testing (CVCT) for prevention. The handover from NGO-sponsored weekend CVCT to government-sponsored services in routine weekday antenatal care (ANC) and individual voluntary testing and counseling (VCT) services in Zambia's two largest cities from 2009-2015 is described.
Government clinic counselors were trained to provide CVCT, and along with community health workers they promoted CVCT services in their clinic and surrounding areas. When client volume exceeded the capacity of on-duty staff in ANC and VCT, non-governmental organization (NGO) subsidies were offered for overtime pay.
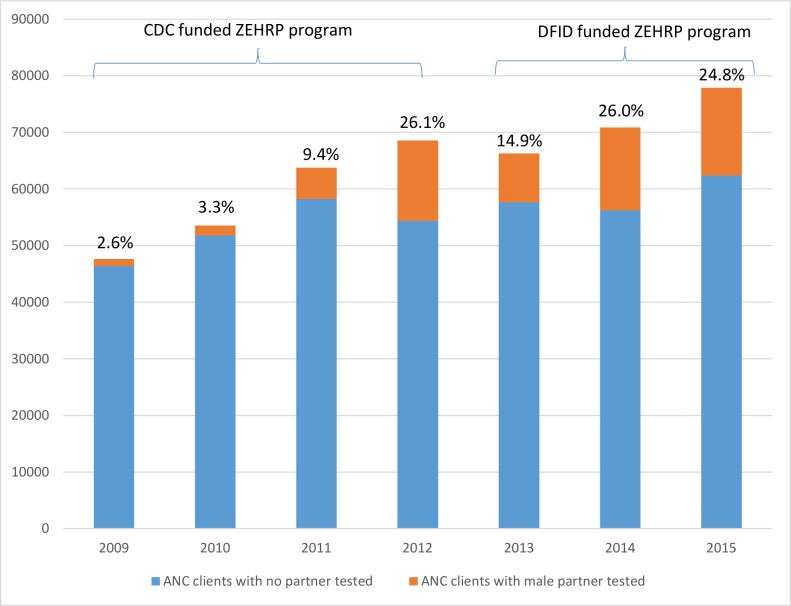
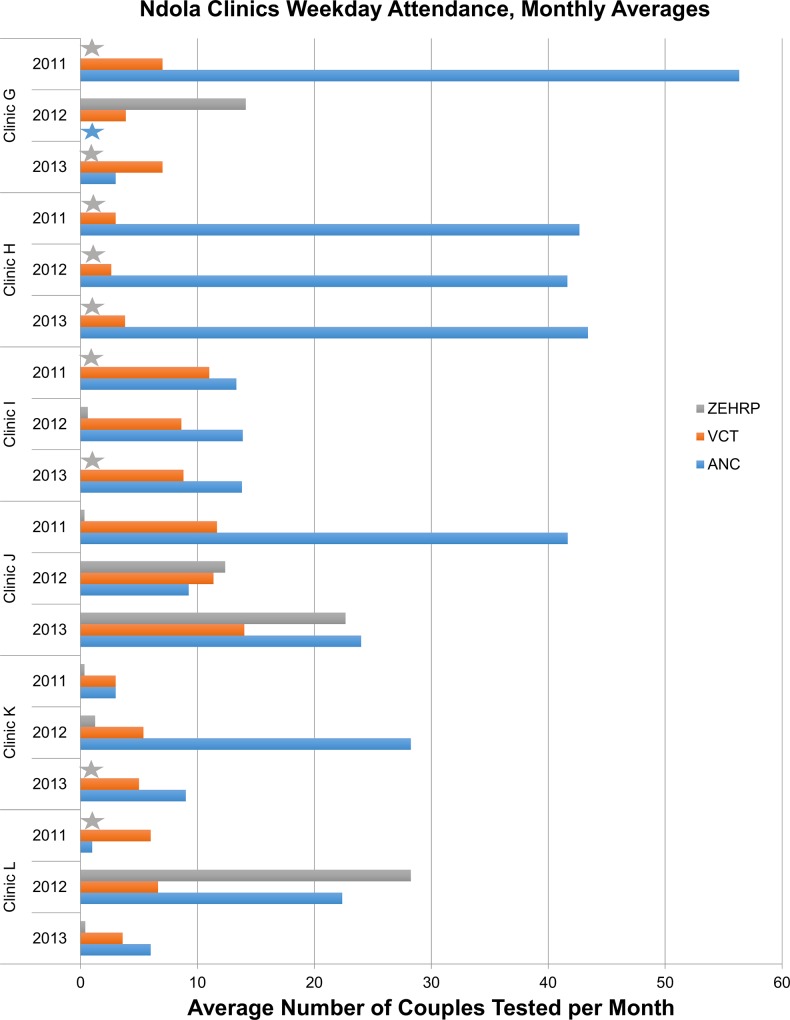
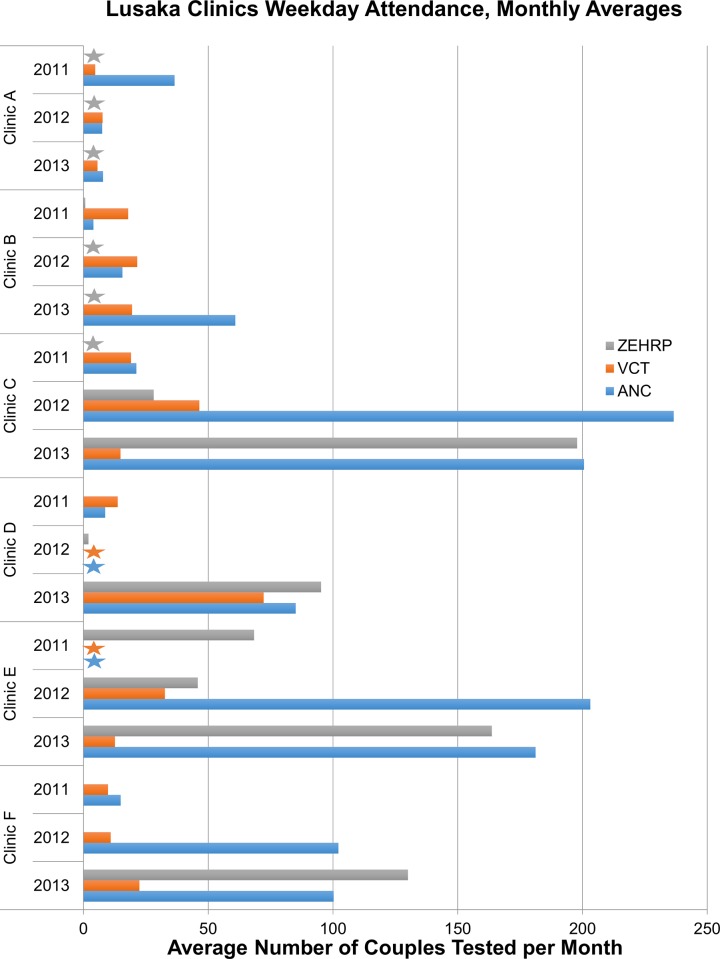
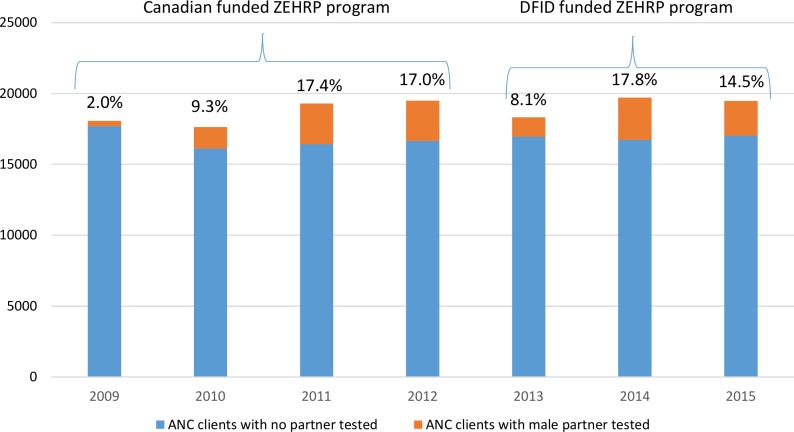
Implementation of routine CVCT services varied greatly by clinic and city. The 12 highest volume clinics were examined further, while 13 clinics had CVCT numbers that were too low to warrant further investigation. In Lusaka, the proportion of pregnant women whose partners were tested rose from 2.6% in 2009 to a peak of 26.2% in 2012 and 24.8% in 2015. Corresponding reports in Ndola were 2.0% in 2009, 17.0% in 2012 and 14.5% in 2015. Obstacles to CVCT included: limited space and staffing, competing priorities, record keeping not adapted for couples, and few resources for promotion and increasing male involvement. Conflicting training models for 'partner testing' with men and women separately vs. CVCT with joint post-test counseling led to confusion in reporting to district health authorities.
A focused and sustained effort will be required to reach a meaningful number of couples with CVCT to prevent heterosexual and perinatal HIV transmission. Establishing targets and timelines, funding for dedicated and appropriately trained staff, adoption of standardized data recording instruments with couple-level indicators, and expansion of community and clinic-based promotions using proven models are recommended.
非洲大多数艾滋病毒感染是已婚/同居成年人感染的,世界卫生组织建议进行夫妻自愿艾滋病毒咨询和检测(CVCT)以预防感染。本文描述了2009年至2015年赞比亚两个最大城市从非政府组织赞助的周末CVCT向政府赞助的常规工作日产前护理(ANC)服务以及个人自愿检测和咨询(VCT)服务的交接情况。
对政府诊所的咨询员进行培训,使其能够提供CVCT服务,并与社区卫生工作者一起在诊所及其周边地区推广CVCT服务。当客户数量超过ANC和VCT值班人员的能力时,提供非政府组织补贴以支付加班费。
常规CVCT服务的实施情况因诊所和城市而异。对12个客户量最高的诊所进行了进一步检查,而另外13个诊所的CVCT数量过低,无需进一步调查。在卢萨卡,其伴侣接受检测的孕妇比例从2009年的2.6%上升到2012年的峰值26.2%,2015年为24.8%。恩多拉的相应报告数据为2009年2.0%,2012年17.0%,2015年14.5%。CVCT的障碍包括:空间和人员有限、优先事项相互竞争、记录保存不适合夫妻、推广和增加男性参与的资源匮乏。针对男性和女性分别进行“伴侣检测”与进行联合检测后咨询的CVCT的培训模式相互冲突,导致向地区卫生当局报告时出现混乱。
需要集中且持续的努力,以使大量夫妻接受CVCT,从而预防异性传播和围产期艾滋病毒传播。建议设定目标和时间表、为专业且经过适当培训的工作人员提供资金、采用带有夫妻层面指标的标准化数据记录工具,并使用经过验证的模式扩大社区和诊所层面的推广活动。