Simsek Melek, Meijer Berrie, Mulder Chris J J, van Bodegraven Adriaan A, de Boer Nanne K H
*Department of Gastroenterology and Hepatology, VU University Medical Center, Amsterdam; and †Department of Gastroenterology, Geriatrics, Internal and Intensive Care Medicine (Co-MIK), Zuyderland Medical Center, Heerlen-Sittard-Geleen, the Netherlands.
Ther Drug Monit. 2017 Dec;39(6):584-588. doi: 10.1097/FTD.0000000000000455.
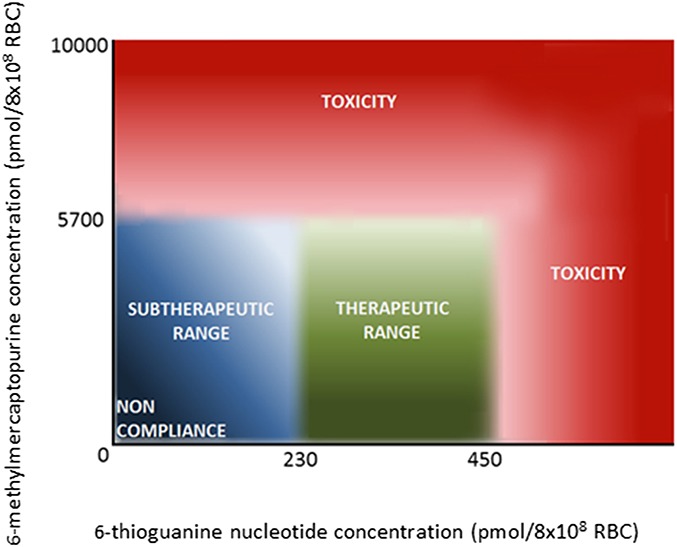
The use of thiopurines in the treatment of inflammatory bowel disease (IBD) can be optimized by the application of therapeutic drug monitoring. In this procedure, 6-thioguanine nucleotides (6-TGN) and 6-methylmercaptopurine (6-MMP) metabolites are monitored and related to therapeutic response and adverse events, respectively. Therapeutic drug monitoring of thiopurines, however, is hampered by several analytical limitations resulting in an impaired translation of metabolite levels to clinical outcome in IBD. Thiopurine metabolism is cell specific and requires nucleated cells and particular enzymes for 6-TGN formation. In the current therapeutic drug monitoring, metabolite levels are assessed in erythrocytes, whereas leukocytes are considered the main target cells of these drugs. Furthermore, currently used methods do not distinguish between active nucleotides and their unwanted residual products. Last, there is a lack of a standardized laboratorial procedure for metabolite assessment regarding the substantial instability of erythrocyte 6-TGN. To improve thiopurine therapy in patients with IBD, it is necessary to understand these limitations and recognize the general misconceptions in this procedure.
通过应用治疗药物监测,可以优化硫嘌呤在炎症性肠病(IBD)治疗中的使用。在此过程中,监测6-硫鸟嘌呤核苷酸(6-TGN)和6-甲基巯基嘌呤(6-MMP)代谢物,并分别将其与治疗反应和不良事件相关联。然而,硫嘌呤的治疗药物监测受到多种分析限制的阻碍,导致代谢物水平与IBD临床结果之间的转化受损。硫嘌呤代谢具有细胞特异性,需要有核细胞和特定酶来形成6-TGN。在当前的治疗药物监测中,在红细胞中评估代谢物水平,而白细胞被认为是这些药物的主要靶细胞。此外,目前使用的方法无法区分活性核苷酸及其不需要的残留产物。最后,由于红细胞6-TGN的显著不稳定性,缺乏用于代谢物评估的标准化实验室程序。为了改善IBD患者的硫嘌呤治疗,有必要了解这些限制并认识到该过程中的常见误解。