Department of Epidemiology, Biostatistics, and Occupational Health, McGill University, Montréal, Canada.
Department of Medicine, McGill University, Montréal, Canada.
J Am Med Inform Assoc. 2018 May 1;25(5):482-495. doi: 10.1093/jamia/ocx107.
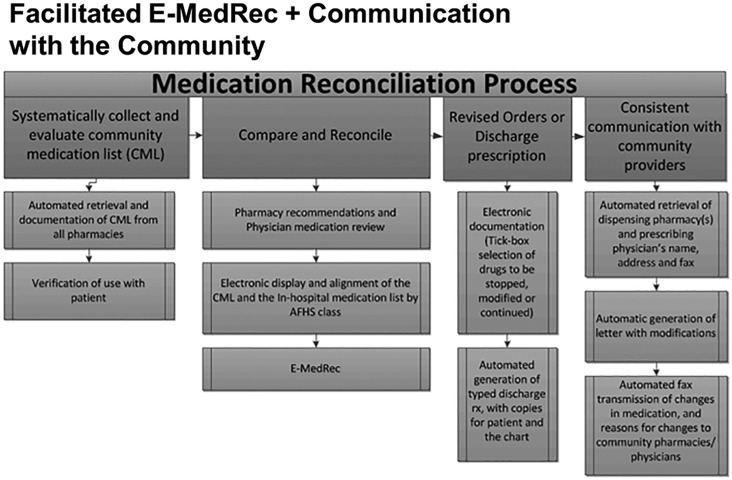
Many countries require hospitals to implement medication reconciliation for accreditation, but the process is resource-intensive, thus adherence is poor. We report on the impact of prepopulating and aligning community and hospital drug lists with data from population-based and hospital-based drug information systems to reduce workload and enhance adoption and use of an e-medication reconciliation application, RightRx.
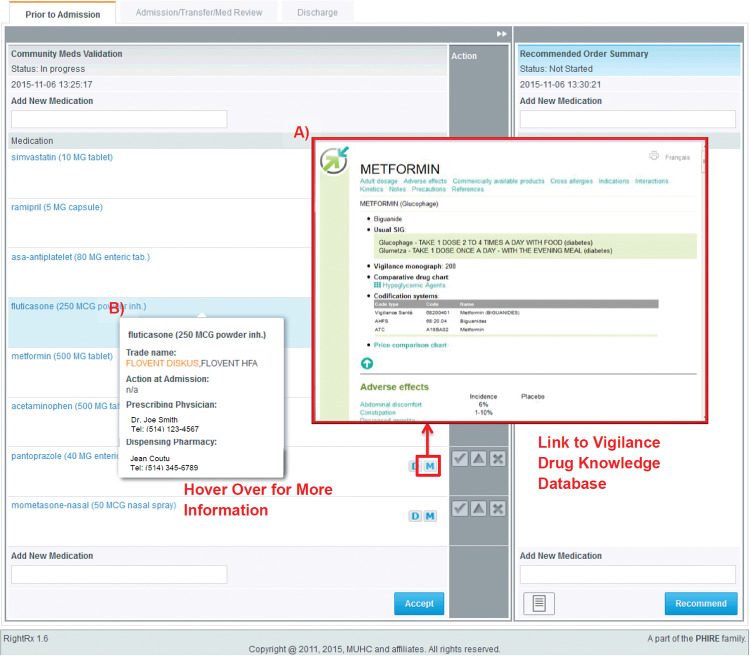
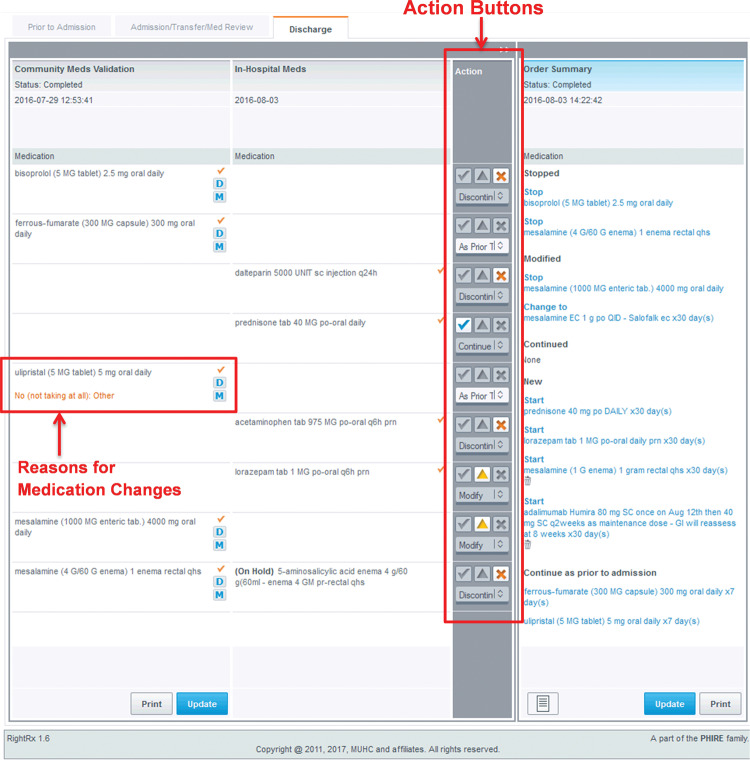
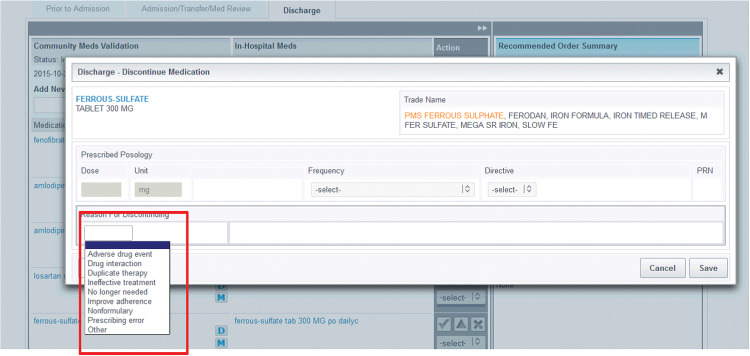
The prototype e-medical reconciliation web-based software was developed for a cluster-randomized trial at the McGill University Health Centre. User-centered design and agile development processes were used to develop features intended to enhance adoption, safety, and efficiency. RightRx was implemented in medical and surgical wards, with support and training provided by unit champions and field staff. The time spent per professional using RightRx was measured, as well as the medication reconciliation completion rates in the intervention and control units during the first 20 months of the trial.
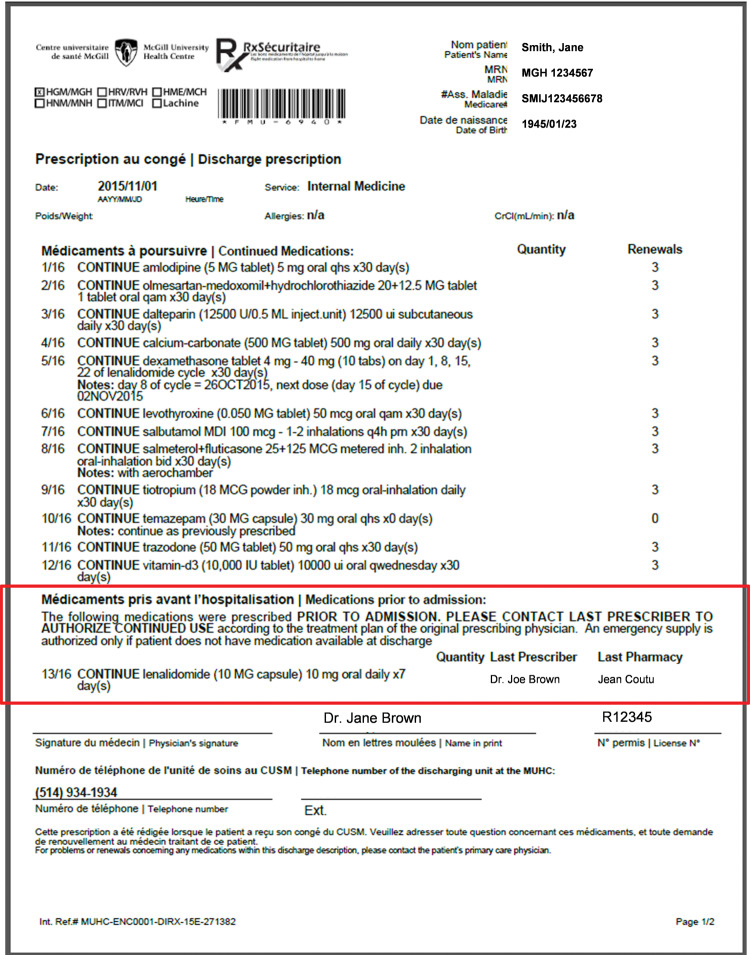
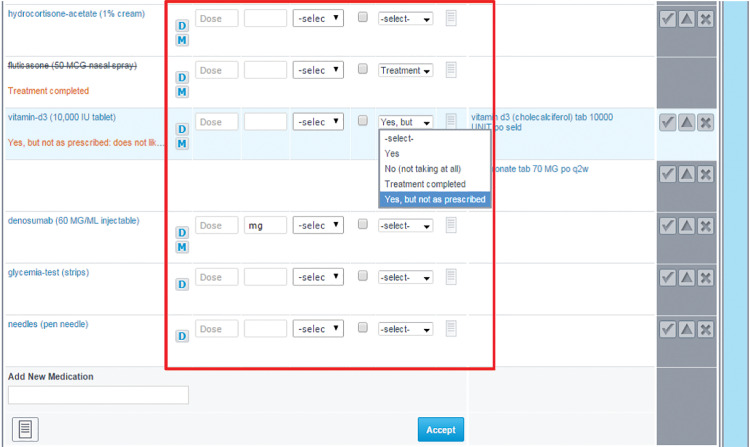
Users identified required modifications to the application, including the need for dose-based prescribing, the role of the discharge physician in prescribing community-based medication, and access to the rationale for medication decisions made during hospitalization. In the intervention units, both physicians and pharmacists were involved in discharge reconciliation, for 96.1% and 71.9% of patients, respectively. Medication reconciliation was completed for 80.7% (surgery) to 96.0% (medicine) of patients in the intervention units, and 0.7% (surgery) to 82.7% of patients in the control units. The odds of completing medication reconciliation were 9 times greater in the intervention compared to control units (odds ratio: 9.0, 95% confidence interval, 7.4-10.9, P < .0001) after adjusting for differences in patient characteristics.
High rates of medication reconciliation completion were achieved with automated prepopulation and alignment of community and hospital medication lists.
许多国家要求医院实施用药核对以达到认证要求,但该过程资源密集,因此依从性较差。我们报告了通过预填充和对齐社区和医院药物清单与基于人群和基于医院的药物信息系统的数据来减少工作量并增强对电子用药核对应用程序 RightRx 的采用和使用的影响。
该基于网络的原型电子用药核对软件是为麦吉尔大学健康中心的一项整群随机试验而开发的。采用以用户为中心的设计和敏捷开发流程来开发旨在增强采用、安全性和效率的功能。RightRx 在医疗和外科病房实施,由单位拥护者和现场工作人员提供支持和培训。测量了每位专业人员使用 RightRx 的时间,以及试验前 20 个月干预和对照组中药物核对完成率。
用户确定了对应用程序的修改要求,包括基于剂量的处方、出院医师在开处社区用药中的作用以及获取住院期间药物决策的理由。在干预病房,医生和药剂师分别参与 96.1%和 71.9%的出院核对。在干预病房,80.7%(外科)至 96.0%(内科)的患者完成了药物核对,而对照组中 0.7%(外科)至 82.7%的患者完成了药物核对。在调整患者特征差异后,干预组与对照组相比,完成药物核对的几率高 9 倍(优势比:9.0,95%置信区间:7.4-10.9,P<0.0001)。
通过自动化预填充和对齐社区和医院用药清单,实现了较高的药物核对完成率。