Department of Epidemiology, Biostatistics and Occupational Health, McGill University, 1020 Pine Avenue West, Montreal, QC H3A 1A2, Canada.
Trials. 2012 Aug 27;13:150. doi: 10.1186/1745-6215-13-150.
Adverse drug events are responsible for up to 7% of all admissions to acute care hospitals. At least 58% of these are preventable, resulting from incomplete drug information, prescribing or dispensing errors, and overuse or underuse of medications. Effective implementation of medication reconciliation is considered essential to reduce preventable adverse drug events occurring at transitions between community and hospital care. An electronically enabled discharge reconciliation process represents an innovative approach to this problem.
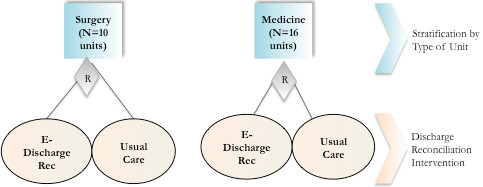
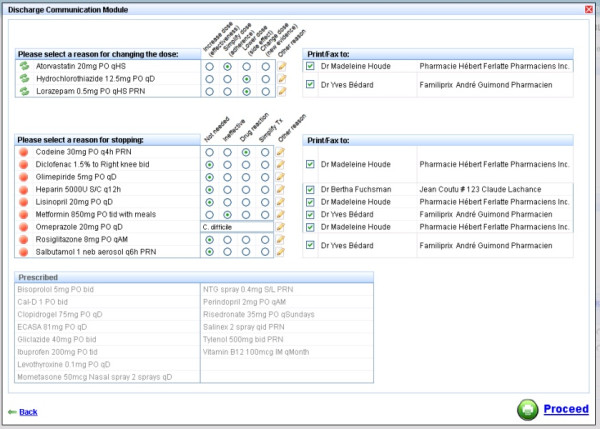
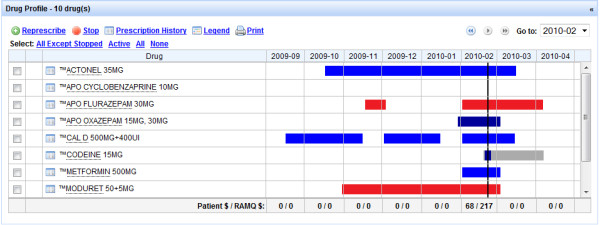
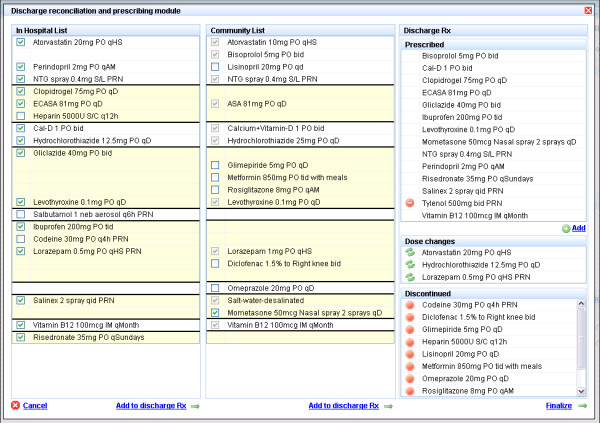
METHODS/DESIGN: Participants will be recruited in Quebec and are eligible for inclusion if they are using prescription medication at admission, covered by the Quebec drug insurance plan, admitted from the community, 18 years or older, admitted to a general or intensive care medical or surgical unit, and discharged alive. A sample size of 3,714 will be required to detect a 5% reduction in adverse drug events. The intervention will comprise electronic retrieval of the community drug list, combined with an electronic discharge reconciliation module and an electronic discharge communication module. The primary outcomes will be adverse drug events occurring 30 days post-discharge, identified by a combination of patient self-report and chart abstraction. All emergency room visits and hospital readmission during this period will be measured as secondary outcomes. A cluster randomization approach will be used to allocate 16 medical and 10 surgical units to electronic discharge reconciliation and communication versus usual care. An intention-to-treat approach will be used to analyse data. Logistic regression will be undertaken within a generalized estimating equation framework to account for clustering within units.
The goal of this prospective trial is to determine if electronically enabled discharge reconciliation will reduce the risk of adverse drug events, emergency room visits and readmissions 30 days post-discharge compared with usual care. We expect that this intervention will improve adherence to medication reconciliation at discharge, the accuracy of the community-based drug history and effective communication of hospital-based treatment changes to community care providers. The results may support policy-directed investments in computerizing and training of hospital staff, generate key requirements for future hospital accreditation standards, and highlight functional requirements for software vendors.
NCT01179867.
药物不良反应导致多达 7%的急性护理医院入院。其中至少 58%是可以预防的,这是由于药物信息不完整、处方或配药错误以及药物过度或不足使用造成的。有效的实施药物重整被认为是减少社区和医院护理之间过渡时发生的可预防药物不良事件的关键。电子启用的出院重整过程是解决此问题的创新方法。
方法/设计:参与者将在魁北克招募,如果他们在入院时使用处方药、受魁北克药物保险计划覆盖、从社区入院、18 岁或以上、入住一般或强化护理医疗或外科病房、并且活着出院,则有资格入选。需要 3714 名样本量才能检测到 5%的药物不良事件减少。干预措施将包括电子检索社区药物清单,结合电子出院重整模块和电子出院通讯模块。主要结局将是出院后 30 天发生的药物不良事件,通过患者自我报告和图表摘录相结合来确定。在此期间所有急诊就诊和医院再入院都将作为次要结局进行测量。将采用集群随机化方法将 16 个医疗和 10 个外科病房分配到电子出院重整和通讯与常规护理相比。将采用意向治疗方法分析数据。将在广义估计方程框架内进行逻辑回归,以解释单位内的聚类。
这项前瞻性试验的目标是确定与常规护理相比,电子启用的出院重整是否会降低出院后 30 天药物不良事件、急诊就诊和再入院的风险。我们预计,这种干预措施将改善出院时的药物重整依从性、社区药物史的准确性以及向社区护理提供者有效传达医院治疗变化。结果可能支持针对医院工作人员计算机化和培训的政策导向投资,为未来的医院认证标准生成关键要求,并突出软件供应商的功能要求。
NCT01179867。