National Intensive Care Surveillance, Quality Secretariat Building, Castle Street Hospital for Women, Colombo 08, Sri Lanka.
Mahidol Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, 3/F, 60th Anniversary Chalermprakiat Building, 420/6 Rajvithi Road, Bangkok, 10400, Thailand.
Crit Care. 2017 Oct 17;21(1):250. doi: 10.1186/s13054-017-1843-6.
Current critical care prognostic models are predominantly developed in high-income countries (HICs) and may not be feasible in intensive care units (ICUs) in lower- and middle-income countries (LMICs). Existing prognostic models cannot be applied without validation in LMICs as the different disease profiles, resource availability, and heterogeneity of the population may limit the transferability of such scores. A major shortcoming in using such models in LMICs is the unavailability of required measurements. This study proposes a simplified critical care prognostic model for use at the time of ICU admission.
This was a prospective study of 3855 patients admitted to 21 ICUs from Bangladesh, India, Nepal, and Sri Lanka who were aged 16 years and over and followed to ICU discharge. Variables captured included patient age, admission characteristics, clinical assessments, laboratory investigations, and treatment measures. Multivariate logistic regression was used to develop three models for ICU mortality prediction: model 1 with clinical, laboratory, and treatment variables; model 2 with clinical and laboratory variables; and model 3, a purely clinical model. Internal validation based on bootstrapping (1000 samples) was used to calculate discrimination (area under the receiver operating characteristic curve (AUC)) and calibration (Hosmer-Lemeshow C-Statistic; higher values indicate poorer calibration). Comparison was made with the Acute Physiology and Chronic Health Evaluation (APACHE) II and Simplified Acute Physiology Score (SAPS) II models.
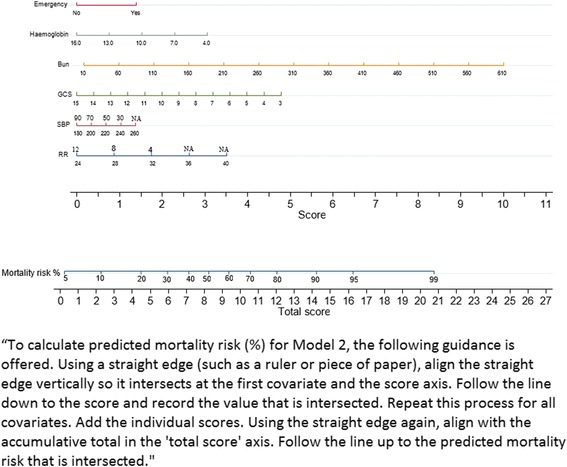
Model 1 recorded the respiratory rate, systolic blood pressure, Glasgow Coma Scale (GCS), blood urea, haemoglobin, mechanical ventilation, and vasopressor use on ICU admission. Model 2, named TropICS (Tropical Intensive Care Score), included emergency surgery, respiratory rate, systolic blood pressure, GCS, blood urea, and haemoglobin. Model 3 included respiratory rate, emergency surgery, and GCS. AUC was 0.818 (95% confidence interval (CI) 0.800-0.835) for model 1, 0.767 (0.741-0.792) for TropICS, and 0.725 (0.688-0.762) for model 3. The Hosmer-Lemeshow C-Statistic p values were less than 0.05 for models 1 and 3 and 0.18 for TropICS. In comparison, when APACHE II and SAPS II were applied to the same dataset, AUC was 0.707 (0.688-0.726) and 0.714 (0.695-0.732) and the C-Statistic was 124.84 (p < 0.001) and 1692.14 (p < 0.001), respectively.
This paper proposes TropICS as the first multinational critical care prognostic model developed in a non-HIC setting.
目前的重症监护预后模型主要是在高收入国家(HICs)开发的,在中低收入国家(LMICs)的重症监护病房(ICUs)中可能不可行。由于不同的疾病谱、资源可用性和人口异质性可能限制这些评分的可转移性,因此在 LMICs 中使用这些模型之前必须进行验证。在 LMICs 中使用此类模型的一个主要缺点是缺乏所需的测量值。本研究提出了一种简化的重症监护预后模型,用于 ICU 入院时使用。
这是一项对来自孟加拉国、印度、尼泊尔和斯里兰卡的 21 个 ICU 收治的 3855 名年龄在 16 岁及以上的患者进行的前瞻性研究,随访至 ICU 出院。捕获的变量包括患者年龄、入院特征、临床评估、实验室检查和治疗措施。使用多变量逻辑回归为 ICU 死亡率预测开发了三个模型:模型 1 包含临床、实验室和治疗变量;模型 2 包含临床和实验室变量;模型 3 是一个纯粹的临床模型。基于 bootstrap(1000 个样本)的内部验证用于计算区分度(受试者工作特征曲线下面积(AUC))和校准(Hosmer-Lemeshow C-Statistic;较高的值表示较差的校准)。与急性生理学和慢性健康评估 (APACHE) II 和简化急性生理学评分 (SAPS) II 模型进行了比较。
模型 1记录了 ICU 入院时的呼吸频率、收缩压、格拉斯哥昏迷量表 (GCS)、血尿素、血红蛋白、机械通气和血管加压素使用情况。模型 2,命名为 TropICS(热带重症监护评分),包括急诊手术、呼吸频率、收缩压、GCS、血尿素和血红蛋白。模型 3 包括呼吸频率、急诊手术和 GCS。模型 1 的 AUC 为 0.818(95%置信区间 (CI) 0.800-0.835),TropICS 为 0.767(0.741-0.792),模型 3 为 0.725(0.688-0.762)。模型 1 和模型 3 的 Hosmer-Lemeshow C-Statistic p 值均小于 0.05,而 TropICS 的 p 值为 0.18。相比之下,当 APACHE II 和 SAPS II 应用于同一数据集时,AUC 分别为 0.707(0.688-0.726)和 0.714(0.695-0.732),C-Statistic 分别为 124.84(p<0.001)和 1692.14(p<0.001)。
本文提出了 TropICS,这是在非 HIC 环境中开发的第一个多国家重症监护预后模型。