Haniffa Rashan, Lubell Yoel, Cooper Ben S, Mohanty Sanjib, Alam Shamsul, Karki Arjun, Pattnaik Rajya, Maswood Ahmed, Haque R, Pangeni Raju, Schultz Marcus J, Dondorp Arjen M
Centre for Tropical Medicine, Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom.
Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
PLoS One. 2017 Mar 14;12(3):e0173483. doi: 10.1371/journal.pone.0173483. eCollection 2017.
To assess the impact on ICU performance of a modular training program in three resource-limited general adult ICUs in India, Bangladesh, and Nepal.
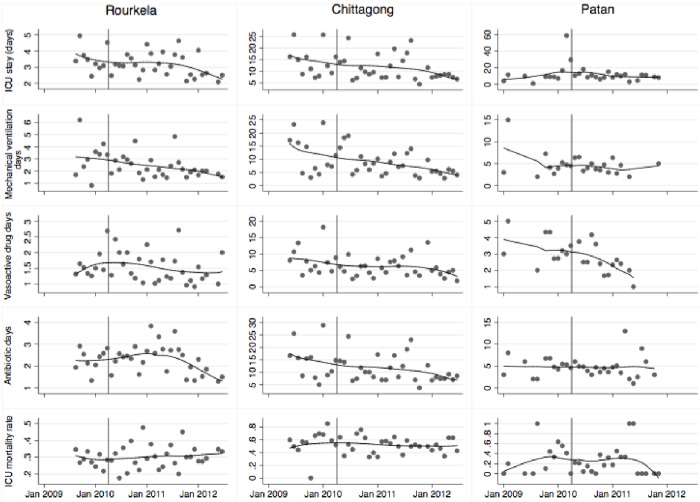
A modular ICU training programme was evaluated using performance indicators from June 2009 to June 2012 using an interrupted time series design with an 8 to 15 month pre-intervention and 18 to 24 month post-intervention period. ICU physicians and nurses trained in Europe and the USA provided training for ICU doctors and nurses. The training program consisted of six modules on basic intensive care practices of 2-3 weeks each over 20 months. The performance indicators consisting of ICU mortality, time to ICU discharge, rate at which patients were discharged alive from the ICU, discontinuation of mechanical ventilation or vasoactive drugs and duration of antibiotic use were extracted. Stepwise changes and changes in trends associated with the intervention were analysed.
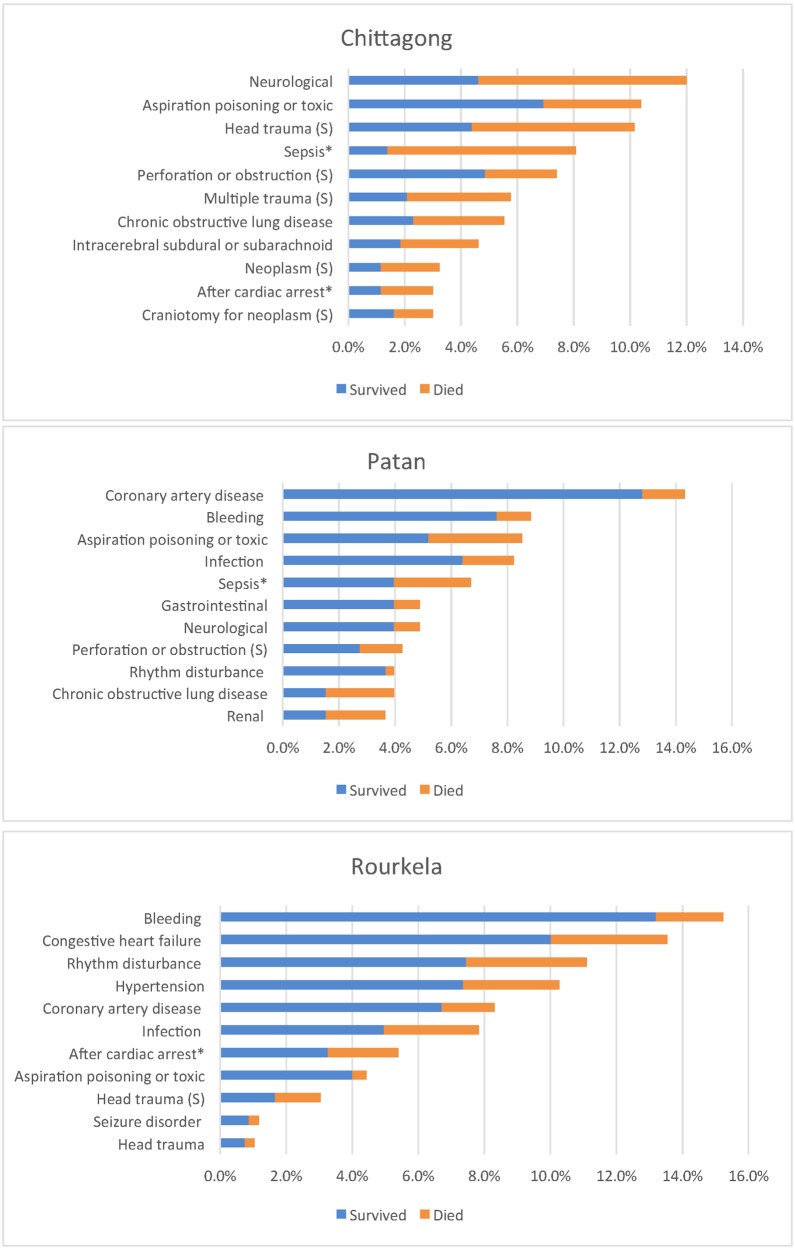
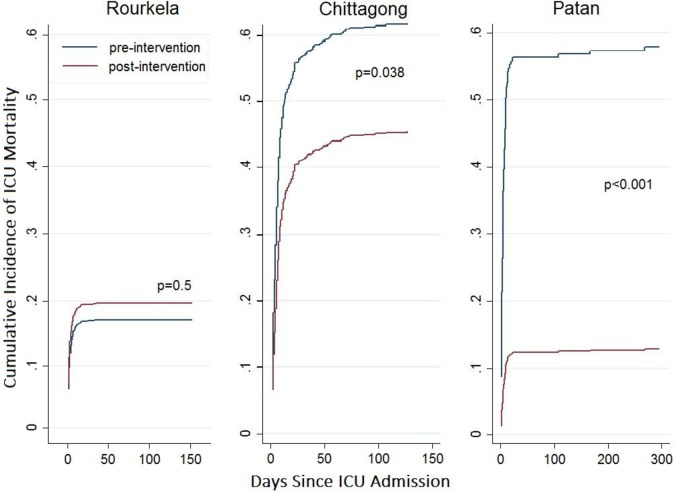
Pre-Training ICU mortality in Rourkela (India), and Patan (Nepal) Chittagong (Bangladesh), was 28%, 41% and 62%, respectively, compared to 30%, 18% and 51% post-intervention. The intervention was associated with a stepwise reduction in cumulative incidence of in-ICU mortality in Chittagong (adjusted subdistribution hazard ratio [aSHR] (95% CI): 0.62 (0.40, 0.97), p = 0.03) and Patan (aSHR 0.16 (0.06, 0.41), p<0.001), but not in Rourkela (aSHR: 1.17 (0.75, 1.82), p = 0.49). The intervention was associated with earlier discontinuation of vasoactive drugs at Rourkela (adjusted hazard ratio for weekly change [aHR] 1.08 (1.03, 1.14), earlier discontinuation of mechanical ventilation in Chittagong (aHR 2.97 (1.24, 7.14), p = 0.02), and earlier ICU discharge in Patan (aHR 1.87 (1.02, 3.43), p = 0.04).
This structured training program was associated with a decrease in ICU mortality in two of three sites and improvement of other performance indicators. A larger cluster randomised study assessing process outcomes and longer-term indicators is warranted.
评估在印度、孟加拉国和尼泊尔的三个资源有限的成人综合重症监护病房(ICU)开展的模块化培训项目对ICU绩效的影响。
采用中断时间序列设计,在2009年6月至2012年6月期间,使用绩效指标对一个模块化ICU培训项目进行评估,干预前期为8至15个月,干预后期为18至24个月。在欧洲和美国接受培训的ICU医生和护士为ICU医生和护士提供培训。培训项目由六个关于基本重症监护实践的模块组成,每个模块为期2 - 3周,共20个月。提取的绩效指标包括ICU死亡率、ICU出院时间、患者从ICU存活出院的比例、机械通气或血管活性药物的停用情况以及抗生素使用时长。分析与干预相关的逐步变化和趋势变化。
在印度鲁尔克拉、尼泊尔帕坦和孟加拉国吉大港,培训前的ICU死亡率分别为28%、41%和62%,干预后分别为30%、18%和51%。该干预与吉大港ICU内死亡率的累积发生率逐步降低相关(调整后亚分布风险比[aSHR](95%置信区间):0.62(0.40,0.97),p = 0.03)以及帕坦(aSHR 0.16(0.06,0.41),p<0.001),但在鲁尔克拉并非如此(aSHR:1.17(0.75,1.82),p = 0.49)。该干预与鲁尔克拉血管活性药物的更早停用相关(每周变化的调整风险比[aHR] 1.08(1.03,1.14)),吉大港机械通气的更早停用(aHR 2.97(1.24,7.14),p = 0.02),以及帕坦ICU的更早出院(aHR 1.87(1.02,3.43),p = 0.04)。
这个结构化培训项目与三个地点中两个地点的ICU死亡率降低以及其他绩效指标的改善相关。有必要开展一项更大规模的整群随机研究来评估过程结果和长期指标。