Department of Critical Care Medicine, Apollo Hospitals, India and Chennai Critical Care Consultants, Chennai, India.
Network for Improving Critical Care Systems and Training, Colombo, Sri Lanka.
PLoS One. 2020 Dec 31;15(12):e0244989. doi: 10.1371/journal.pone.0244989. eCollection 2020.
The use of severity of illness scoring systems such as the Acute Physiology and Chronic Health Evaluation in lower-middle income settings comes with important limitations, primarily due to data burden, missingness of key variables and lack of resources. To overcome these challenges, in Asia, a simplified model, designated as e-TropICS was previously developed. We sought to externally validate this model using data from a multi-centre critical care registry in India.
Seven ICUs from the Indian Registry of IntenSive care(IRIS) contributed data to this study. Patients > 18 years of age with an ICU length of stay > 6 hours were included. Data including age, gender, co-morbidity, diagnostic category, type of admission, vital signs, laboratory measurements and outcomes were collected for all admissions. e-TropICS was calculated as per original methods. The area under the receiver operator characteristic curve was used to express the model's power to discriminate between survivors and non-survivors. For all tests of significance, a 2-sided P less than or equal to 0.05 was considered to be significant. AUROC values were considered poor when ≤ to 0.70, adequate between 0.71 to 0.80, good between 0.81 to 0.90, and excellent at 0.91 or higher. Calibration was assessed using Hosmer-Lemeshow C -statistic.
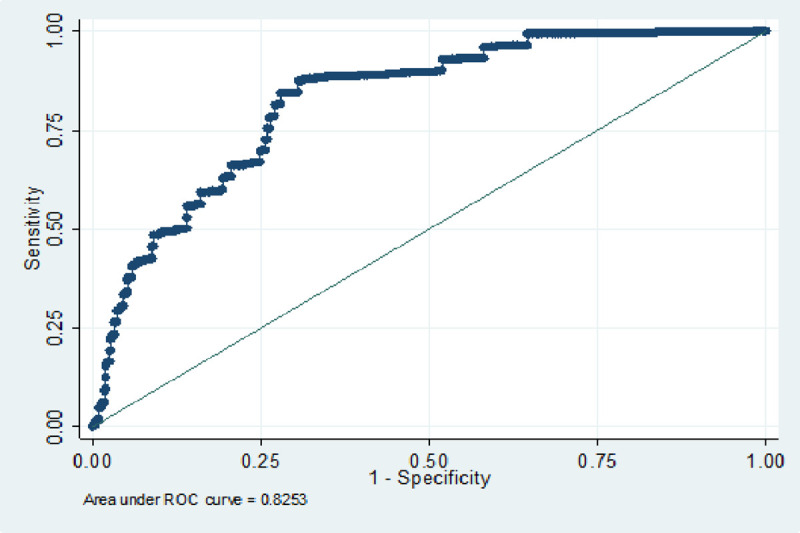
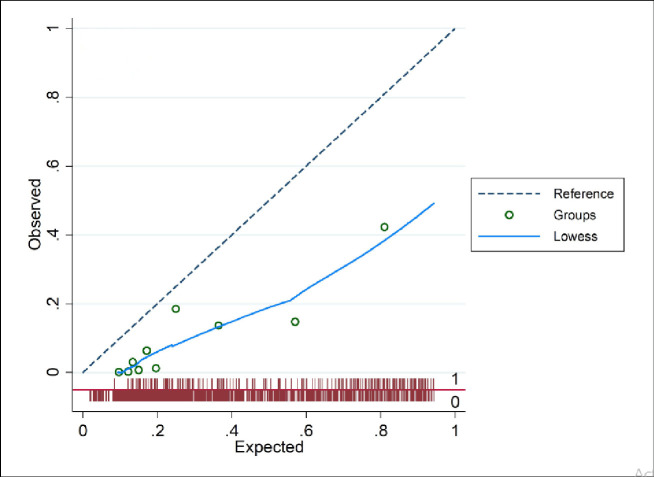
We included data from 2062 consecutive patient episodes. The median age of the cohort was 60 and predominantly male (n = 1350, 65.47%). Mechanical Ventilation and vasopressors were administered at admission in 504 (24.44%) and 423 (20.51%) patients respectively. Overall, mortality at ICU discharge was 10.28% (n = 212). Discrimination (AUC) for the e-TropICS model was 0.83 (95% CI 0.812-0.839) with an HL C statistic p value of < 0.05. The best sensitivity and specificity (84% and 72% respectively) were achieved with the model at an optimal cut-off for probability of 0.29.
e-TropICS has utility in the care of critically unwell patients in the South Asia region with good discriminative capacity. Further refinement of calibration in larger datasets from India and across the South-East Asia region will help in improving model performance.
在中低收入国家使用严重程度评分系统(如急性生理学和慢性健康评估)存在重要限制,主要是由于数据负担、关键变量缺失和资源不足。为了克服这些挑战,亚洲开发了一种简化模型,称为 e-TropICS。我们试图使用印度多中心重症监护登记处的数据来对此模型进行外部验证。
来自印度重症监护登记处(IRIS)的 7 个 ICU 为这项研究提供了数据。纳入年龄>18 岁、入住 ICU 时间>6 小时的患者。所有患者的入院时均采集了年龄、性别、合并症、诊断类别、入院类型、生命体征、实验室检查和结局等数据。根据原始方法计算 e-TropICS。使用接受者操作特征曲线下的面积来表示该模型区分幸存者和非幸存者的能力。所有显著性检验均采用双侧 P 值≤0.05。AUROC 值<0.70 表示较差,0.71-0.80 表示尚可,0.81-0.90 表示良好,0.91 或更高表示优秀。采用 Hosmer-Lemeshow C 统计量评估校准度。
共纳入 2062 例连续患者病例。队列的中位年龄为 60 岁,主要为男性(n = 1350,65.47%)。504 例(24.44%)和 423 例(20.51%)患者在入 ICU 时分别接受了机械通气和血管加压药治疗。总体而言,ICU 出院时的死亡率为 10.28%(n = 212)。e-TropICS 模型的区分度(AUC)为 0.83(95%CI 0.812-0.839),Hosmer-Lemeshow C 统计量 p 值<0.05。该模型的最佳灵敏度和特异性分别为 84%和 72%,概率最佳截断值为 0.29。
e-TropICS 在南亚地区对重症患者具有良好的区分能力,具有一定的实用性。在印度和东南亚地区更大的数据集进一步细化校准将有助于提高模型性能。