Xue Ying, Goodwin James S, Adhikari Deepak, Raji Mukaila A, Kuo Yong-Fang
1 University of Rochester School of Nursing, Rochester, NY, USA.
2 University of Texas Medical Branch, Galveston, TX, USA.
J Prim Care Community Health. 2017 Oct;8(4):256-263. doi: 10.1177/2150131917736634. Epub 2017 Oct 19.
To document the temporal trends in alternative primary care models in which physicians, nurse practitioners (NPs), or physician assistants (PAs) engaged in care provision to the elderly, and examine the role of these models in serving elders with multiple chronic conditions and those residing in rural and health professional shortage areas (HPSAs).
Serial cross-sectional analysis of Medicare claims data for years 2008, 2011, and 2014.
Primary care outpatient setting.
Medicare fee-for-service beneficiaries who had at least 1 primary care office visit in each study year. The sample size is 2 471 498.
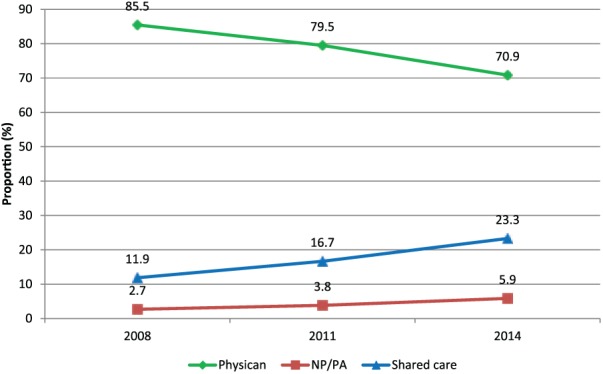
Physician model-Medicare beneficiary's primary care office visits in a year were conducted exclusively by physicians; shared care model-conducted by a group of professionals that included physicians and either NPs or PAs or both; NP/PA model: conducted either by NPs or PAs or both.
There was a decrease in the physician model (85.5% to 70.9%) and an increase in the shared care model (11.9% to 23.3%) and NP/PA model (2.7% to 5.9%) from 2008 to 2014. Compared with the physician model, the adjusted odds ratio (AOR) of receiving NP/PA care was 3.97 (95% CI 3.80-4.14) in rural and 1.26 (95% CI 1.23-1.29) in HPSAs; and the AOR of receiving shared care was 1.66 (95% CI 1.61-1.72) and 1.14 (95% CI 1.13-1.15), respectively. Beneficiaries with 3 or more chronic conditions were most likely to received shared care (AOR = 1.67, 95% CI 1.65-1.70).
The increase in shared care practice signifies a shift toward bolstering capacity of the primary care delivery system to serve elderly populations with growing chronic disease burden and to improve access to care in rural and HPSAs.
记录医生、执业护士(NP)或医师助理(PA)为老年人提供护理的替代初级保健模式的时间趋势,并研究这些模式在为患有多种慢性病的老年人以及居住在农村和医疗专业人员短缺地区(HPSA)的老年人提供服务中的作用。
对2008年、2011年和2014年医疗保险索赔数据进行系列横断面分析。
初级保健门诊环境。
在每个研究年度至少有1次初级保健门诊就诊的医疗保险按服务付费受益人。样本量为2471498。
医生模式——医疗保险受益人的年度初级保健门诊就诊仅由医生进行;共享护理模式——由包括医生以及NP或PA或两者的一组专业人员进行;NP/PA模式:由NP或PA或两者进行。
从2008年到2014年,医生模式有所下降(从85.5%降至70.9%),共享护理模式(从11.9%增至23.3%)和NP/PA模式(从2.7%增至5.9%)有所增加。与医生模式相比,在农村接受NP/PA护理的调整优势比(AOR)为3.97(95%可信区间3.80 - 4.14),在HPSA为1.26(95%可信区间1.23 - 1.29);接受共享护理的AOR分别为1.66(95%可信区间1.61 - 1.72)和1.14(95%可信区间1.13 - 1.15)。患有3种或更多慢性病的受益人最有可能接受共享护理(AOR = 1.67,95%可信区间1.65 - 1.70)。
共享护理实践的增加表明初级保健提供系统正朝着增强服务慢性病负担不断增加的老年人群体的能力以及改善农村和HPSA地区医疗服务可及性的方向转变。