Department of Neurology, The First Affiliated Hospital, Chongqing Medical University, Chongqing 400016, China.
Chin Med J (Engl). 2017 Oct 20;130(20):2489-2497. doi: 10.4103/0366-6999.216401.
To provide a comprehensive and latest overview of susceptibility-weighted imaging (SWI) in the application of thrombolysis in acute ischemic stroke, and to update the decision-making effect and clinical value of SWI on identifying stroke patients suitable for thrombolytic therapy and possible benefits and risks followed.
Literatures referred to this review were collected from PubMed, Medline, and EMBASE published till May 2017, using the search terms including susceptibility-weighted imaging, gradient-echo, T2*, thrombolysis, recombinant tissue plasminogen activator (rt-PA), thrombolytic therapy, and stroke.
Papers in English or with available English abstracts were considered, with no limitation of study design. References were also identified from the bibliographies of identified articles and the authors' files.
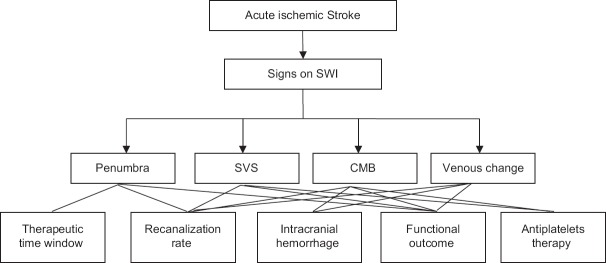
SWI is of guiding significance for thrombolytic therapy in stroke patients, it can predict the location and length of thrombus and ischemic penumbra. It is worthy of noting that susceptibility vessel sign (SVS) on SWI can be used to predict recanalization after thrombolytic therapy and whether it is better to implement endovascular thrombolectomy in combination or alone. SWI is sensitive in detecting cerebral microbleed (CMB), and CMB might not be a contraindication for thrombolytic therapy, yet CMBs in multiple foci could possibly be related to intracranial hemorrhage (ICH) after thrombolysis. SVS and CMB on SWI sequence are of instructive value in performing antiplatelet therapy after thrombolytic therapy. Cerebral venous change on SWI is related to lower recanalization rate and poor outcome after thrombolysis.
It seems that SWI can be applied to guide individualized thrombolytic therapies and assist clinicians in making better decisions by weighing benefits and risks. However, there still exist controversies about the relationship between signs on SWI and thrombolytic therapy.
提供关于磁敏感加权成像(SWI)在急性缺血性脑卒中溶栓治疗中应用的全面、最新综述,更新 SWI 对识别适合溶栓治疗的脑卒中患者的决策效果和临床价值,以及可能的获益和风险。
检索 2017 年 5 月以前PubMed、Medline 和 EMBASE 中有关磁敏感加权成像、梯度回波、T2*、溶栓、重组组织型纤溶酶原激活剂(rt-PA)、溶栓治疗和脑卒中的文献,检索词包括 susceptibility-weighted imaging、gradient-echo、T2*、thrombolysis、recombinant tissue plasminogen activator (rt-PA)、thrombolytic therapy 和 stroke。
纳入英语文献或有英文摘要的文献,设计类型不限。还从确定的文章的参考文献和作者文件中确定参考文献。
SWI 对脑卒中患者的溶栓治疗具有指导意义,可预测血栓和缺血半暗带的位置和长度。值得注意的是,SWI 上的易损血管征(SVS)可用于预测溶栓治疗后的再通以及联合或单独实施血管内血栓切除术是否更好。SWI 对脑微出血(CMB)的检测很敏感,CMB 可能不是溶栓治疗的禁忌证,但多个部位的 CMB 可能与溶栓后颅内出血(ICH)有关。SWI 序列上的 SVS 和 CMB 在溶栓后抗血小板治疗中有指导价值。SWI 上的脑静脉改变与溶栓后再通率低和预后不良有关。
SWI 似乎可用于指导个体化溶栓治疗,并通过权衡获益和风险帮助临床医生做出更好的决策。然而,SWI 上的征象与溶栓治疗之间的关系仍存在争议。