Exponent, Inc., 3440 Market St, Suite 600, Philadelphia, PA, USA.
Oklahoma Spine, Edmond, OK, USA.
Osteoporos Int. 2018 Feb;29(2):375-383. doi: 10.1007/s00198-017-4281-z. Epub 2017 Oct 24.
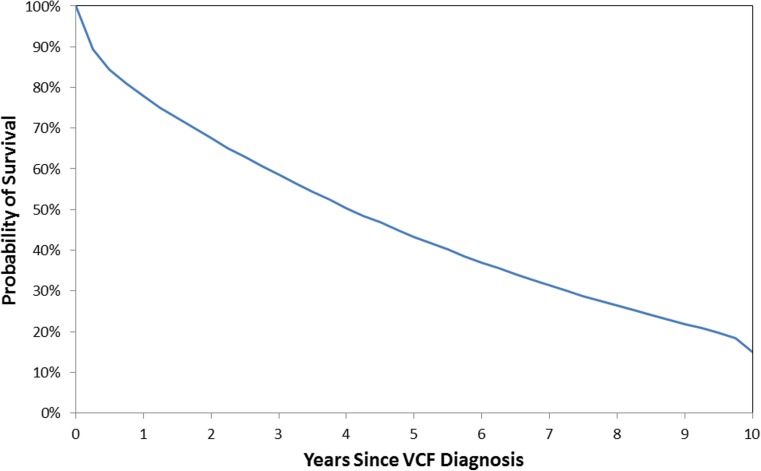
The 5-year period following 2009 saw a steep reduction in vertebral augmentation volume and was associated with elevated mortality risk in vertebral compression fracture (VCF) patients. The risk of mortality following a VCF diagnosis was 85.1% at 10 years and was found to be lower for balloon kyphoplasty (BKP) and vertebroplasty (VP) patients.
BKP and VP are associated with lower mortality risks than non-surgical management (NSM) of VCF. VP versus sham trials published in 2009 sparked controversy over its effectiveness, leading to diminished referral volumes. We hypothesized that lower BKP/VP utilization would lead to a greater mortality risk for VCF patients.
BKP/VP utilization was evaluated for VCF patients in the 100% US Medicare data set (2005-2014). Survival and morbidity were analyzed by the Kaplan-Meier method and compared between NSM, BKP, and VP using Cox regression with adjustment by propensity score and various factors.
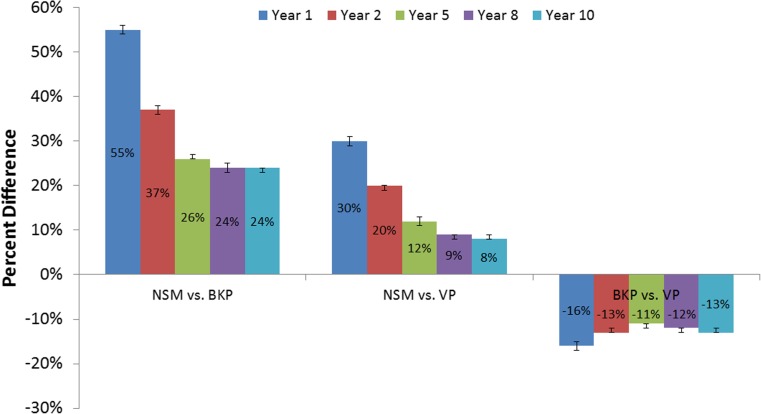
The cohort included 261,756 BKP (12.6%) and 117,232 VP (5.6%) patients, comprising 20% of the VCF patient population in 2005, peaking at 24% in 2007-2008, and declining to 14% in 2014. The propensity-adjusted mortality risk for VCF patients was 4% (95% CI, 3-4%; p < 0.001) greater in 2010-2014 versus 2005-2009. The 10-year risk of mortality for the overall cohort was 85.1%. BKP and VP cohorts had a 19% (95% CI, 19-19%; p < 0.001) and 7% (95% CI, 7-8%; p < 0.001) lower propensity-adjusted 10-year mortality risk than the NSM cohort, respectively. The BKP cohort had a 13% (95% CI, 12-13%; p < 0.001) lower propensity-adjusted 10-year mortality risk than the VP cohort.
Changes in treatment patterns following the 2009 VP publications led to fewer augmentation procedures. In turn, the 5-year period following 2009 was associated with elevated mortality risk in VCF patients. This provides insight into the implications of treatment pattern changes and associated mortality risks.
2009 年后的 5 年期间,椎体增强量急剧减少,与椎体压缩性骨折(VCF)患者的死亡率升高有关。VCF 诊断后 10 年的死亡率为 85.1%,球囊扩张椎体后凸成形术(BKP)和椎体成形术(VP)患者的死亡率较低。
BKP 和 VP 与非手术治疗(NSM)相比,与较低的死亡率风险相关。2009 年发表的 VP 与假手术对照试验引发了其疗效的争议,导致转诊量减少。我们假设,BKP/VP 利用率的降低将导致 VCF 患者的死亡风险增加。
在 100%美国医疗保险数据集(2005-2014 年)中评估 VCF 患者的 BKP/VP 使用率。采用 Kaplan-Meier 法分析生存率和发病率,并采用 Cox 回归比较 NSM、BKP 和 VP 之间的差异,同时通过倾向评分和各种因素进行调整。
该队列包括 261756 例 BKP(12.6%)和 117232 例 VP(5.6%)患者,占 2005 年 VCF 患者人群的 20%,在 2007-2008 年达到峰值的 24%,并在 2014 年降至 14%。与 2005-2009 年相比,2010-2014 年 VCF 患者的死亡率风险增加了 4%(95%CI,3-4%;p<0.001)。整个队列的 10 年死亡率为 85.1%。BKP 和 VP 队列的 10 年死亡率分别比 NSM 队列低 19%(95%CI,19-19%;p<0.001)和 7%(95%CI,7-8%;p<0.001)。与 VP 队列相比,BKP 队列的 10 年死亡率风险低 13%(95%CI,12-13%;p<0.001)。
2009 年 VP 出版物后的治疗模式变化导致了较少的增强程序。反过来,2009 年后的 5 年期间与 VCF 患者的死亡率升高有关。这为我们了解治疗模式变化及其相关的死亡率风险提供了线索。