Gommans D H Frank, Cramer G Etienne, Bakker Jeannette, Dieker Hendrik-Jan, Michels Michelle, Fouraux Michael A, Marcelis Carlo L M, Verheugt Freek W A, Timmermans Janneke, Brouwer Marc A, Kofflard Marcel J M
Department of Cardiology, Radboud University Medical Center, Nijmegen, The Netherlands.
Department of Cardiology 616, Radboud University Medical Center, Geert Grooteplein 10, P.O. Box 9101, 6525 GA, Nijmegen, The Netherlands.
Int J Cardiovasc Imaging. 2018 Jan;34(1):113-120. doi: 10.1007/s10554-017-1252-6. Epub 2017 Oct 23.
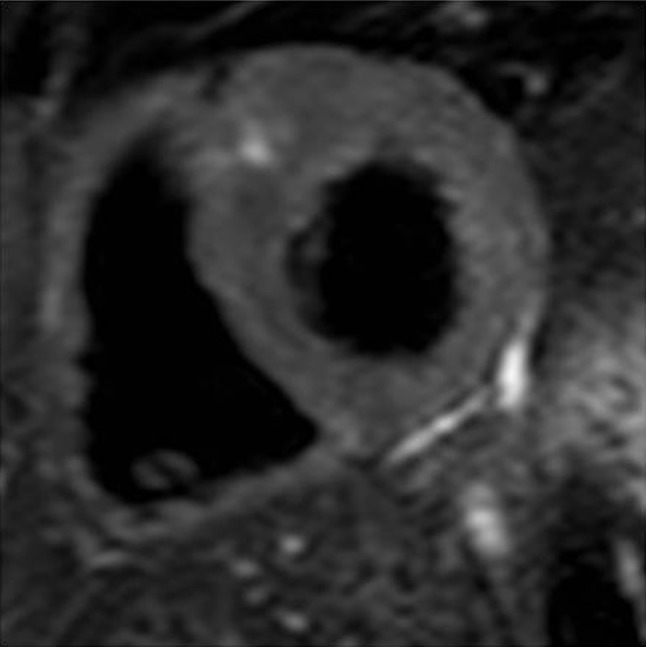
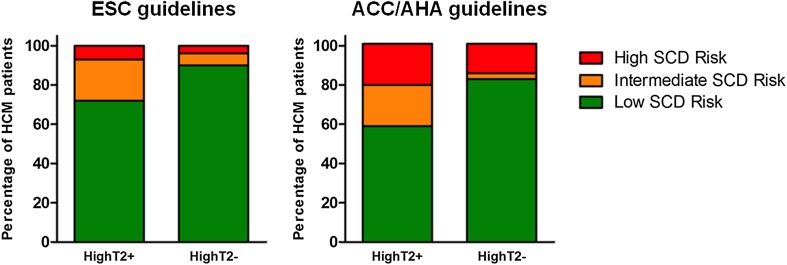
In search of improved risk stratification in hypertrophic cardiomyopathy (HCM), CMR imaging has been implicated as a potential tool for prediction of sudden cardiac death (SCD). In follow-up of the promising results with extensive late gadolinium enhancement (LGE), high signal-intensity on T2-weighted imaging (HighT2) has become subject of interest given its association with markers of adverse disease progression, such as LGE, elevated troponin and non-sustained ventricular tachycardia. In lack of follow-up cohorts, we initiated an exploratory study on the association between HighT2 and the internationally defined risk categories of SCD. In a cohort of 109 HCM patients from a multicenter study on CMR imaging and biomarkers, we estimated the 5-year SCD risk (HCM Risk-SCD model). Patients were categorized as low (< 4%), intermediate (≥ 4-<6%) or high (≥ 6%) risk. In addition, risk categorization according to the ACC/AHA guidelines was performed. HighT2 was present in 27% (29/109). Patients with HighT2 were more often at an intermediate-high risk of SCD according to the European (28 vs. 10%, p = .032) and American guidelines (41 vs. 18%, p = .010) compared to those without HighT2. The estimated 5-year SCD risk of our cohort was 1.9% (IQR 1.3-2.9%), and projected SCD rates were higher in patients with than without HighT2 (2.8 vs. 1.8%, p = .002). In conclusion, HCM patients with HighT2 were more likely to be intermediate-high risk, with projected SCD rates that were 1.5 fold higher than in patients without HighT2. These pilot findings call for corroborative studies with more intermediate-high risk HCM patients and clinical follow-up to assess whether HighT2 may have additional value to current risk stratification.
为了改善肥厚型心肌病(HCM)的风险分层,心脏磁共振成像(CMR)被认为是预测心源性猝死(SCD)的一种潜在工具。在对广泛延迟钆增强(LGE)的良好结果进行随访时,鉴于T2加权成像上的高信号强度(HighT2)与不良疾病进展标志物(如LGE、肌钙蛋白升高和非持续性室性心动过速)相关,它已成为研究热点。由于缺乏随访队列,我们开展了一项关于HighT2与国际定义的SCD风险类别之间关联的探索性研究。在一项关于CMR成像和生物标志物的多中心研究的109例HCM患者队列中,我们估计了5年SCD风险(HCM风险-SCD模型)。患者被分为低风险(<4%)、中风险(≥4%-<6%)或高风险(≥6%)。此外,根据美国心脏病学会/美国心脏协会(ACC/AHA)指南进行了风险分类。27%(29/109)的患者存在HighT2。与无HighT2的患者相比,根据欧洲指南(28%对10%,p = 0.032)和美国指南(41%对18%,p = 0.010),有HighT2的患者更常处于SCD的中高风险。我们队列的估计5年SCD风险为1.9%(四分位间距1.3 - 2.9%),有HighT2的患者预计SCD发生率高于无HighT2的患者(2.8%对1.8%,p = 0.002)。总之,有HighT2的HCM患者更可能处于中高风险,预计SCD发生率比无HighT2的患者高1.5倍。这些初步发现需要更多中高风险HCM患者的验证性研究和临床随访,以评估HighT2是否可能对当前风险分层具有额外价值。