Hudson Mark, Radwan Amr, Di Maggio Paola, Cipelli Riccardo, Ryder Stephen D, Dillon John F, Cash William Jonathan, Przemioslo Robert T, Wright Mark, Shawcross Debbie L, Jalan Rajiv, Saksena Sushma, Allison Michael, Richardson Paul, Farrington Elizabeth, Aspinall Richard J
Liver Unit, Freeman Hospital, Newcastle upon Tyne, UK.
UK Medical Affairs, Norgine, Harefield, UK.
Frontline Gastroenterol. 2017 Oct;8(4):243-251. doi: 10.1136/flgastro-2016-100792. Epub 2017 Apr 7.
To compare all-cause and liver-related hospital resource use in the 6 and 12 months pre-rifaximin-α and post-rifaximin-α initiation in UK patients with hepatic encephalopathy (HE).
A UK multicentre, retrospective, observational study. Patients' medical records were reviewed for demographics, clinical outcomes and adverse events (AEs) to rifaximin-α. Details of hospital admissions/attendances in the 6 and 12 months pre-rifaximin-α and post-rifaximin-α initiation were extracted from hospital electronic databases.
13 National Health Service centres.
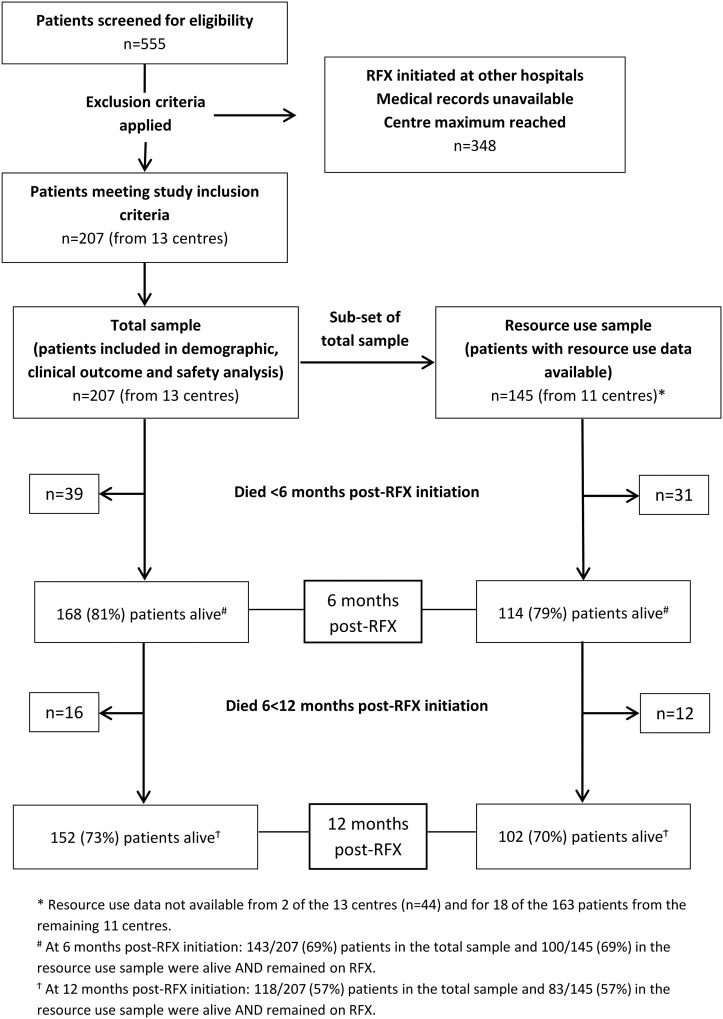
207 patients with HE who initiated rifaximin-α between July 2008 and May 2014. Hospital resource use data were available for 145/207 patients.
Change in mean number of liver-related hospital bed days/patient (total and critical care) between the 6 months pre-rifaximin-α and post-rifaximin-α initiation.
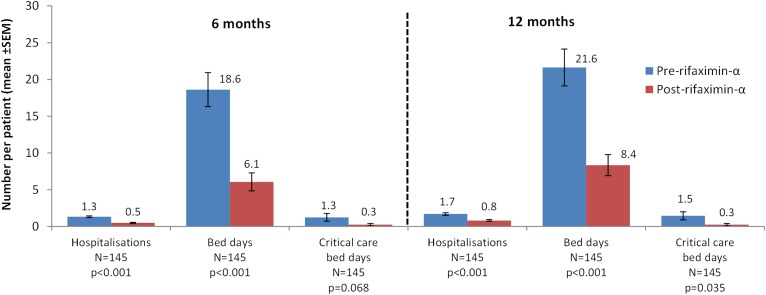
Comparing the 6 months pre-rifaximin-α and post-rifaximin-α initiation in alive patients at the end of the observation period (N=114): there were significant reductions in the mean number of hospitalisations/patient (liver-related 1.3 to 0.5, p<0.001; all-cause 1.9 to 0.9, p<0.001), hospital bed days/patient (liver-related 17.8 to 6.8, p<0.001; all-cause 25.4 to 10.6, p<0.001), 30-day hospital readmissions/patient (liver-related 0.5 to 0.2, p=0.039; all-cause 0.8 to 0.4, p=0.024) and emergency department (ED) attendances/patient (all-cause, 1.0 to 0.5, p<0.001). The mean critical care bed days/patient reduced significantly for all-cause admissions (1.3 to 0.3, p=0.049); non-significant reduction for liver-related admissions. 4% of patients (9/207) developed AEs.
In UK clinical practice, treatment with rifaximin-α for HE is well-tolerated and associated with significant reductions in hospitalisations, bed days (including critical care), ED attendances and 30-day readmissions.
比较英国肝性脑病(HE)患者在开始使用利福昔明-α之前6个月和12个月以及开始使用之后6个月和12个月的全因和肝脏相关医院资源使用情况。
一项英国多中心、回顾性、观察性研究。查阅患者病历以获取人口统计学信息、临床结局以及对利福昔明-α的不良事件(AE)。从医院电子数据库中提取开始使用利福昔明-α之前6个月和12个月以及之后6个月和12个月的住院/就诊详细信息。
13个国民医疗服务中心。
207例在2008年7月至2014年5月期间开始使用利福昔明-α的HE患者。145/207例患者有医院资源使用数据。
开始使用利福昔明-α之前6个月和之后6个月之间每位患者肝脏相关住院天数(总计和重症监护)的变化。
比较观察期结束时存活患者(N = 114)开始使用利福昔明-α之前6个月和之后6个月的情况:每位患者的住院次数显著减少(肝脏相关从1.3次降至0.5次,p<0.001;全因从1.9次降至0.9次,p<0.001),住院天数(肝脏相关从17.8天降至6.8天,p<0.001;全因从25.4天降至10.6天,p<0.001),30天内再次住院率(肝脏相关从0.5降至0.2,p = 0.039;全因从0.8降至0.4,p = 0.024)以及急诊就诊率(全因,从1.0降至0.5,p<0.001)。全因住院的每位患者平均重症监护天数显著减少(从1.3天降至0.3天,p = 0.049);肝脏相关住院的减少不显著。4%的患者(9/207)出现不良事件。
在英国临床实践中,利福昔明-α治疗HE耐受性良好,且与住院次数、住院天数(包括重症监护)、急诊就诊次数和30天内再入院率的显著降低相关。