Wandling Michael W, Ko Clifford Y, Bankey Paul E, Cribari Chris, Cryer H Gill, Diaz Jose J, Duane Therese M, Hameed S Morad, Hutter Matthew M, Metzler Michael H, Regner Justin L, Reilly Patrick M, Reines H David, Sperry Jason L, Staudenmayer Kristan L, Utter Garth H, Crandall Marie L, Bilimoria Karl Y, Nathens Avery B
From the Department of Surgery (M.W.W., K.Y.B.), Northwestern University Feinberg School of Medicine; Division of Research and Optimal Patient Care, (M.W.W., C.Y.K., K.Y.B., A.B.N.), American College of Surgeons, Chicago, IL; Department of Surgery (C.Y.K.), University of California-Los Angeles; Department of Surgery (C.Y.K.), VA Greater Los Angeles Healthcare System, Los Angeles, CA; Division of Acute Care Surgery, Department of Surgery (P.E.B.), University of Rochester Medical Center, Rochester, NY; Division of Acute Care Surgery, Department of Surgery (C.C., M.H.M.), Medical Center of the Rockies, University of Colorado Health, Loveland, CO; Department of Surgery (H.G.C.), Ronald Reagan UCLA (University of California, Los Angeles) Medical Center, UCLA David Geffen School of Medicine, Los Angeles, CA; Division of Acute Care Surgery, Program in Trauma (J.J.D.), R Adams Cowley Shock Trauma Center, University of Maryland, Baltimore, MD; Department of Surgery (T.M.D.), John Peter Smith Health Network, Fort Worth, TX; Section of Trauma and Acute Care Surgery, Department of Surgery (S.M.H.), University of British Columbia, Vancouver, BC, Canada; Department of Surgery (M.M.H.), Massachusetts General Hospital, Boston, MA; Department of Surgery (J.L.R.), Scott and White Memorial Hospital, Temple, TX; Division of Traumatology, Surgical Critical Care, and Emergency Surgery, Department of Surgery (P.M.R.), University of Pennsylvania Perelman School of Medicine, Philadelphia, PA,; Department of Surgery (H.D.R.), Inova Fairfax Hospital, Falls Church, VA; Division of Trauma and General Surgery, Department of Surgery (J.L.S.), University of Pittsburgh Medical Center, Pittsburgh, PA; Department of Surgery (K.L.S.), Stanford University, Stanford; Department of Surgery (G.H.U.), University of California, Davis, Medical Center, Sacramento, CA; Department of Surgery (M.L.C.), University of Florida College of Medicine-Jacksonville, Jacksonville, FL; and Department of Surgery (A.B.N.), Sunnybrook Health Sciences Centre, University of Toronto, Toronto, ON, Canada.
J Trauma Acute Care Surg. 2017 Nov;83(5):837-845. doi: 10.1097/TA.0000000000001670.
Patients managed nonoperatively have been excluded from risk-adjusted benchmarking programs, including the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP). Consequently, optimal performance evaluation is not possible for specialties like emergency general surgery (EGS) where nonoperative management is common. We developed a multi-institutional EGS clinical data registry within ACS NSQIP that includes patients managed nonoperatively to evaluate variability in nonoperative care across hospitals and identify gaps in performance assessment that occur when only operative cases are considered.
Using ACS NSQIP infrastructure and methodology, surgical consultations for acute appendicitis, acute cholecystitis, and small bowel obstruction (SBO) were sampled at 13 hospitals that volunteered to participate in the EGS clinical data registry. Standard NSQIP variables and 16 EGS-specific variables were abstracted with 30-day follow-up. To determine the influence of complications in nonoperative patients, rates of adverse outcomes were identified, and hospitals were ranked by performance with and then without including nonoperative cases.
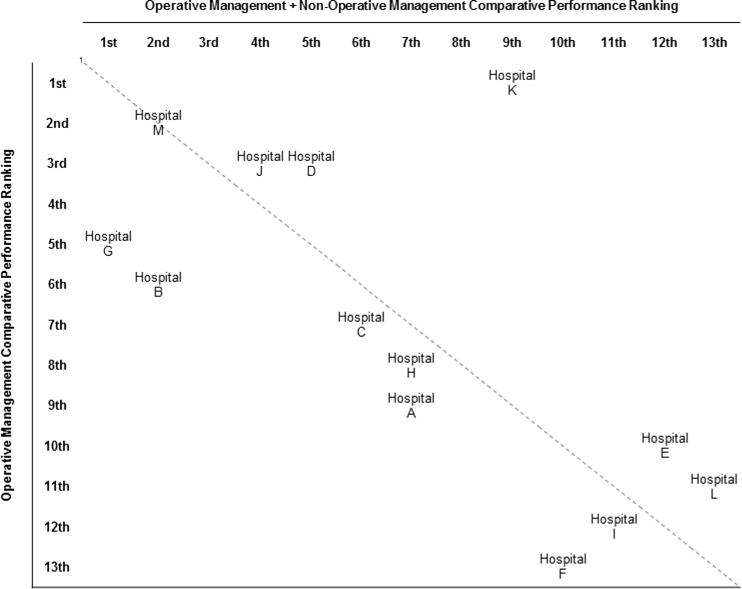
Two thousand ninety-one patients with EGS diagnoses were included, 46.6% with appendicitis, 24.3% with cholecystitis, and 29.1% with SBO. The overall rate of nonoperative management was 27.4%, 6.6% for appendicitis, 16.5% for cholecystitis, and 69.9% for SBO. Despite comprising only 27.4% of patients in the EGS pilot, nonoperative management accounted for 67.7% of deaths, 34.3% of serious morbidities, and 41.8% of hospital readmissions. After adjusting for patient characteristics and hospital diagnosis mix, addition of nonoperative management to hospital performance assessment resulted in 12 of 13 hospitals changing performance rank, with four hospitals changing by three or more positions.
This study identifies a gap in performance evaluation when nonoperative patients are excluded from surgical quality assessment and demonstrates the feasibility of incorporating nonoperative care into existing surgical quality initiatives. Broadening the scope of hospital performance assessment to include nonoperative management creates an opportunity to improve the care of all surgical patients, not just those who have an operation.
Care management, level IV; Epidemiologic, level III.
接受非手术治疗的患者被排除在风险调整后的基准评估项目之外,包括美国外科医师学会(ACS)的国家外科质量改进项目(NSQIP)。因此,对于像急诊普通外科(EGS)这样非手术治疗很常见的专科,无法进行最佳绩效评估。我们在ACS NSQIP内建立了一个多机构的EGS临床数据登记处,纳入接受非手术治疗的患者,以评估各医院非手术治疗的差异,并找出仅考虑手术病例时绩效评估中存在的差距。
利用ACS NSQIP的基础设施和方法,在13家自愿参与EGS临床数据登记处的医院抽取了急性阑尾炎、急性胆囊炎和小肠梗阻(SBO)的外科会诊病例。提取了标准的NSQIP变量和16个EGS特定变量,并进行了30天的随访。为确定非手术患者并发症的影响,确定了不良结局发生率,并对医院进行了绩效排名,先是包括非手术病例,然后不包括非手术病例。
纳入了2091例EGS诊断患者,其中46.6%为阑尾炎,24.3%为胆囊炎,29.1%为SBO。非手术治疗的总体比例为27.4%,阑尾炎为6.6%,胆囊炎为16.5%,SBO为69.9%。尽管在EGS试点中仅占患者的27.4%,但非手术治疗导致了67.7%的死亡、34.3%的严重并发症和41.8%的医院再入院。在对患者特征和医院诊断组合进行调整后,将非手术治疗纳入医院绩效评估,导致13家医院中有12家改变了绩效排名,其中4家医院的排名变动了三个或更多位置。
本研究发现了在手术质量评估中排除非手术患者时绩效评估存在的差距,并证明了将非手术治疗纳入现有手术质量计划的可行性。扩大医院绩效评估范围以包括非手术治疗,为改善所有外科患者的护理创造了机会,而不仅仅是那些接受手术的患者。
护理管理,IV级;流行病学,III级。