van Dijk S T, Daniels L, Nio C Y, Somers I, van Geloven A A W, Boermeester M A
Department of Surgery, Academic Medical Center, Meibergdreef 9, 1100 DD, PO Box 22660, Amsterdam, The Netherlands.
Department of Radiology, Academic Medical Center, Amsterdam, The Netherlands.
Int J Colorectal Dis. 2017 Dec;32(12):1693-1698. doi: 10.1007/s00384-017-2919-0. Epub 2017 Oct 26.
Since outpatient treatment and omitting antibiotics for uncomplicated acute colonic diverticulitis have been proven to be safe in the majority of patients, selection of patients that may not be suited for this treatment strategy becomes an important topic. The aim of this study is to identify computed tomography (CT) imaging predictors for a complicated disease course of initially uncomplicated acute diverticulitis.
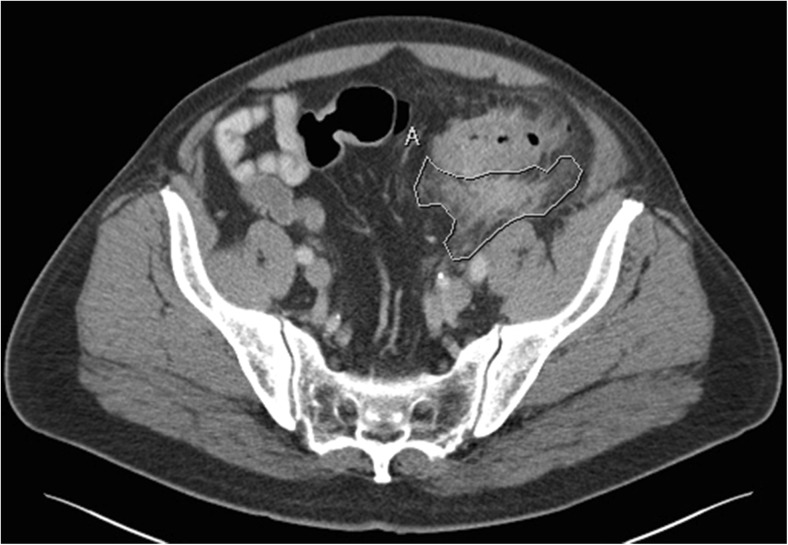
CT imaging from a randomized controlled trial (DIABOLO study) of an observational vs. antibiotic treatment strategy of first-episode uncomplicated acute diverticulitis patients was re-evaluated. For each patient that developed complicated diverticulitis within 90 days after randomization, two patients with an uncomplicated disease course were randomly selected. Two abdominal radiologists, blinded for outcomes, independently re-evaluated all CTs.
Of the 528 patients in the DIABOLO trial, 16 patients developed complications (abscess > 5 cm, perforation, bowel obstruction) within 90 days after randomization. In the group with a complicated course of initially uncomplicated diverticulitis, more patients with fluid collections (25 vs. 0%; p = 0.009) and a longer inflamed colon segment (86 ± 26 mm vs. 65 ± 21 mm; p = 0.007) were observed compared to an uncomplicated course of disease. Pericolic extraluminal air was no predictive factor.
Fluid collections and to a lesser extent the length of the inflamed colon segment may serve as predictive factors on initial CT for a complicated disease course in patients with uncomplicated acute colonic diverticulitis. These findings may aid in the selection of patients not suitable for outpatient treatment and treatment without antibiotics.
由于门诊治疗以及对单纯性急性结肠憩室炎不使用抗生素已被证明对大多数患者是安全的,因此选择可能不适合这种治疗策略的患者成为一个重要课题。本研究的目的是确定初发单纯性急性憩室炎病情复杂的计算机断层扫描(CT)影像预测指标。
对一项关于初发单纯性急性憩室炎患者观察性与抗生素治疗策略的随机对照试验(DIABOLO研究)的CT影像进行重新评估。对于随机分组后90天内发生复杂性憩室炎的每位患者,随机选择两名病情未复杂化的患者。两名对结果不知情的腹部放射科医生独立重新评估所有CT影像。
在DIABOLO试验的528例患者中,16例在随机分组后90天内出现并发症(脓肿>5cm、穿孔、肠梗阻)。在初发单纯性憩室炎病情复杂的组中,与病情未复杂化的组相比,观察到更多有积液的患者(25%对0%;p=0.009)以及更长的炎症结肠段(86±26mm对65±21mm;p=0.007)。结肠周围腔外气体不是预测因素。
积液以及在较小程度上炎症结肠段的长度可作为初发CT上单纯性急性结肠憩室炎患者病情复杂的预测因素。这些发现可能有助于选择不适合门诊治疗和不使用抗生素治疗的患者。