Centre for Pharmacoepidemiology and Drug Safety, Division of Pharmacy and Optometry, School of Health Sciences, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester, UK.
Dermatology Centre, Salford Royal NHS Foundation Trust, The University of Manchester, Manchester Academic Health Science Centre, Manchester, UK; Division of Musculoskeletal and Dermatological Sciences, School of Biological Sciences and NIHR Manchester Biomedical Research Centre, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester, UK.
J Invest Dermatol. 2018 Apr;138(4):775-784. doi: 10.1016/j.jid.2017.09.044. Epub 2017 Dec 6.
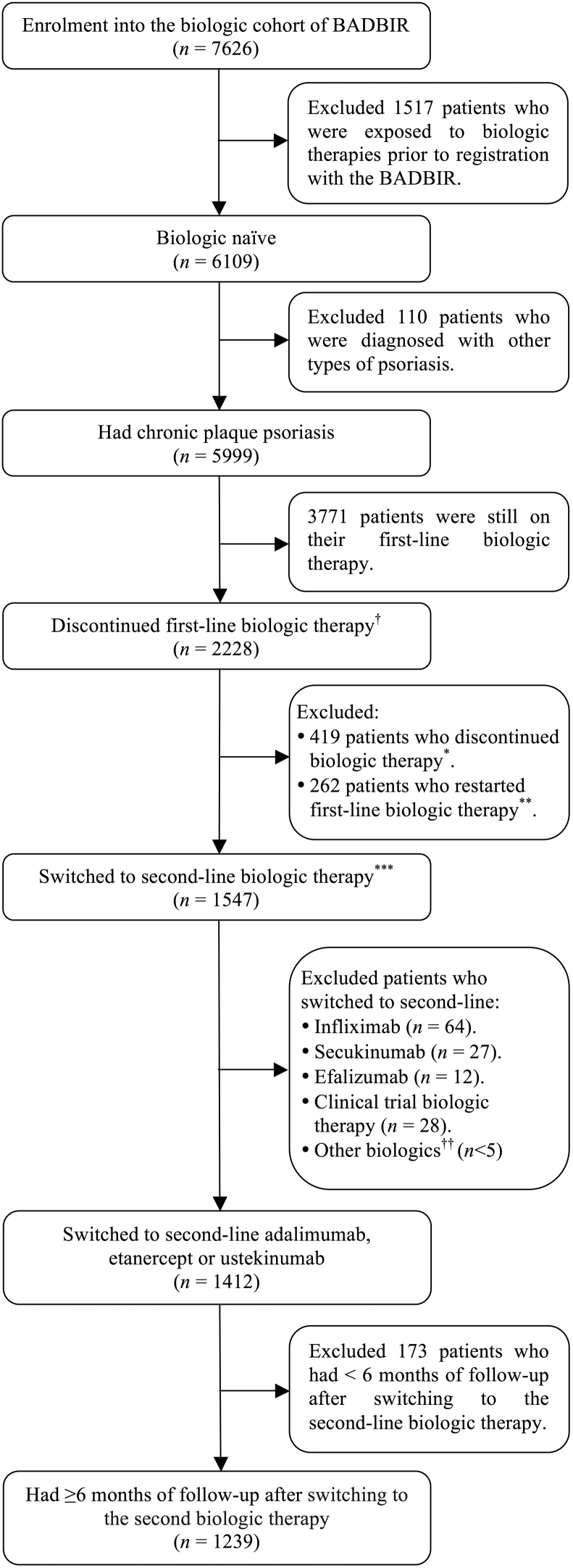
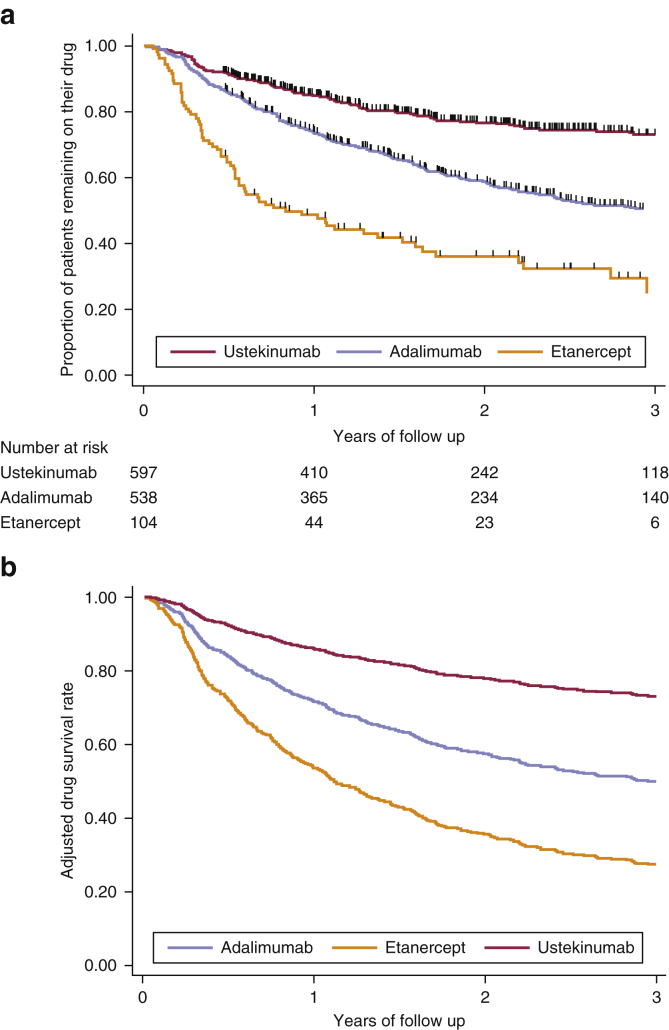
Little is known about the drug survival of second-line biologic therapies for psoriasis in routine clinical practice. We assessed drug survival of second-line biologic therapies and estimated the risk of recurrent discontinuation due to adverse events or ineffectiveness in patients with psoriasis who had failed a first biologic therapy and switched to a second in a large, multicenter pharmacovigilance registry (n = 1,239; adalimumab, n = 538; etanercept, n = 104; ustekinumab, n = 597). The overall drug survival rate in the first year after switching was 77% (95% confidence interval = 74-79%), falling to 58% (55-61%) in the third year. Female sex, multiple comorbidities, concomitant therapy with cyclosporine, and a high Psoriasis Area and Severity Index at switching to the second-line biologic therapy were predictors of overall discontinuation (multivariable Cox proportional hazard model). Compared to adalimumab, patients receiving etanercept were more likely to discontinue therapy (hazard ratio = 1.87, 95% confidence interval = 1.24-2.83), whereas patients receiving ustekinumab were more likely to persist (hazard ratio = 0.46; 95% confidence interval = 0.33-0.64). Discontinuation of the first biologic therapy because of adverse events was associated with an increased rate of second drug discontinuation because of adverse events (hazard ratio = 2.55; 95% confidence interval = 1.50-4.32). In conclusion, drug survival rates differed among biologic therapies and decreased over time; second-line discontinuation because of adverse events was more common among those who discontinued first-line treatment for this reason. The results of this study should support clinical decision making when choosing second-line biologic therapy for patients with psoriasis.
关于银屑病患者在接受一线生物制剂治疗失败后转换为二线生物制剂治疗时的药物生存情况,目前在常规临床实践中知之甚少。本研究评估了银屑病患者在接受一线生物制剂治疗失败后转换为二线生物制剂治疗时的药物生存情况,并估计了因不良事件或无效而再次停药的风险(n=1239;阿达木单抗,n=538;依那西普,n=104;乌司奴单抗,n=597)。转换后第一年的总体药物生存率为 77%(95%置信区间[CI]:74-79%),第三年降至 58%(55-61%)。女性、多种合并症、转换为二线生物制剂治疗时同时接受环孢素治疗以及较高的银屑病面积和严重程度指数(PASI)是总体停药的预测因素(多变量 Cox 比例风险模型)。与阿达木单抗相比,接受依那西普治疗的患者更有可能停止治疗(风险比[HR]=1.87,95%CI:1.24-2.83),而接受乌司奴单抗治疗的患者更有可能持续治疗(HR=0.46;95%CI:0.33-0.64)。由于不良事件而停止使用一线生物制剂治疗与因不良事件而再次停止二线药物治疗的发生率增加相关(HR=2.55;95%CI:1.50-4.32)。总之,不同生物制剂治疗的药物生存率不同,且随时间推移而降低;由于不良事件而停止二线治疗的情况在因该原因停止一线治疗的患者中更为常见。本研究结果应为临床医生为银屑病患者选择二线生物制剂治疗提供决策支持。