Tickell-Painter Maya, Maayan Nicola, Saunders Rachel, Pace Cheryl, Sinclair David
Department of Clinical Sciences, Liverpool School of Tropical Medicine, Liverpool, UK.
Cochrane Database Syst Rev. 2017 Oct 30;10(10):CD006491. doi: 10.1002/14651858.CD006491.pub4.
Mefloquine is one of four antimalarial agents commonly recommended for preventing malaria in travellers to malaria-endemic areas. Despite its high efficacy, there is controversy about its psychological side effects.
To summarize the efficacy and safety of mefloquine used as prophylaxis for malaria in travellers.
We searched the Cochrane Infectious Diseases Group Specialized Register; the Cochrane Central Register of Controlled Trials (CENTRAL), published on the Cochrane Library; MEDLINE; Embase (OVID); TOXLINE (https://toxnet.nlm.nih.gov/newtoxnet/toxline.htm); and LILACS. We also searched the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP; http://www.who.int/ictrp/en/) and ClinicalTrials.gov (https://clinicaltrials.gov/ct2/home) for trials in progress, using 'mefloquine', 'Lariam', and 'malaria' as search terms. The search date was 22 June 2017.
We included randomized controlled trials (for efficacy and safety) and non-randomized cohort studies (for safety). We compared prophylactic mefloquine with placebo, no treatment, or an alternative recommended antimalarial agent. Our study populations included all adults and children, including pregnant women.
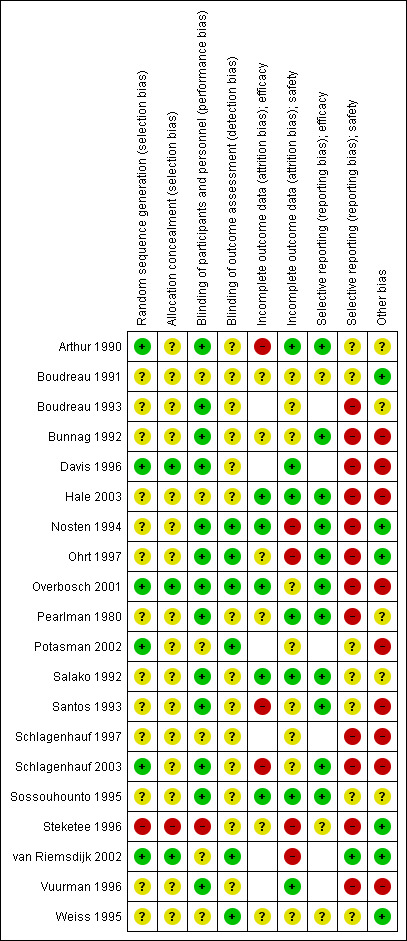
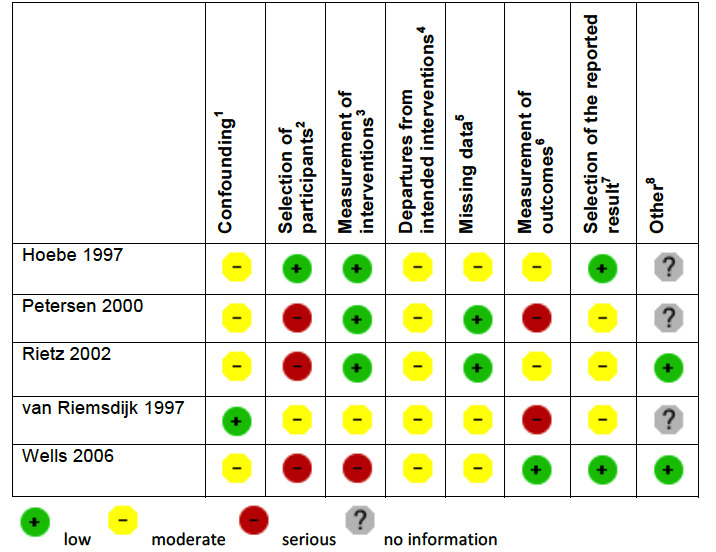
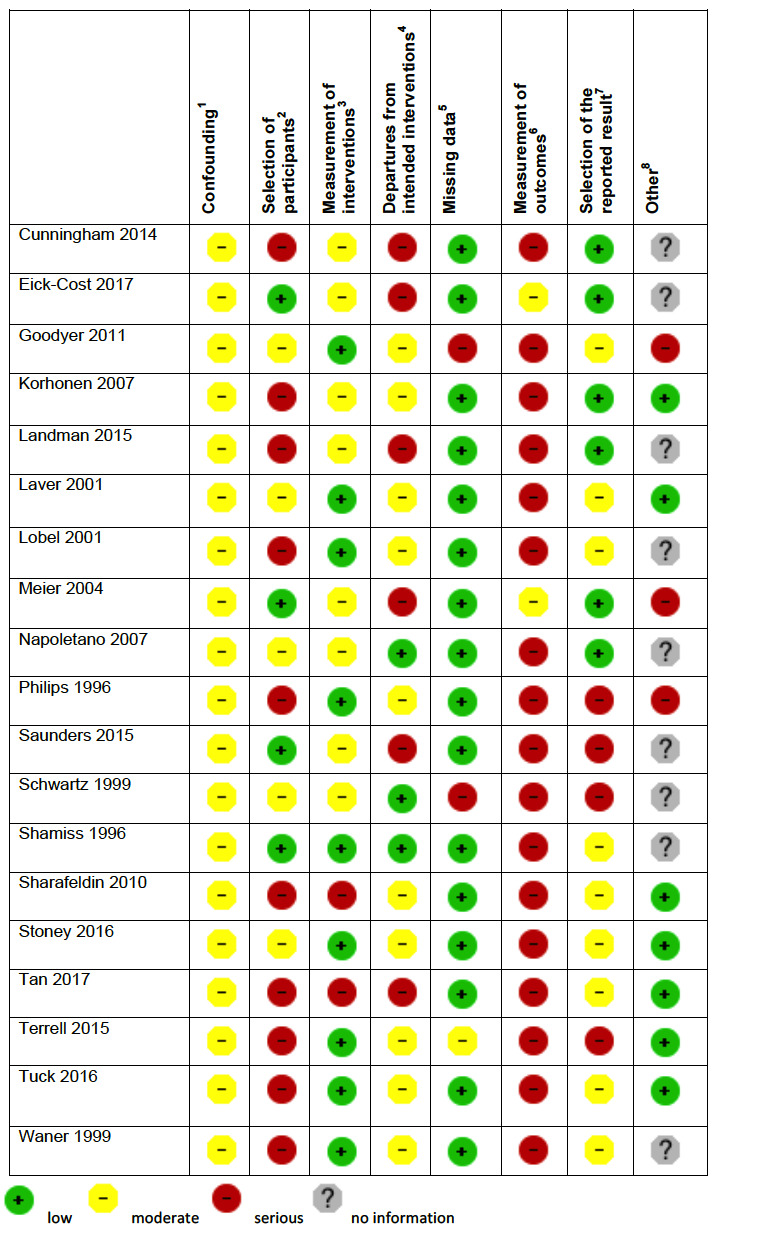
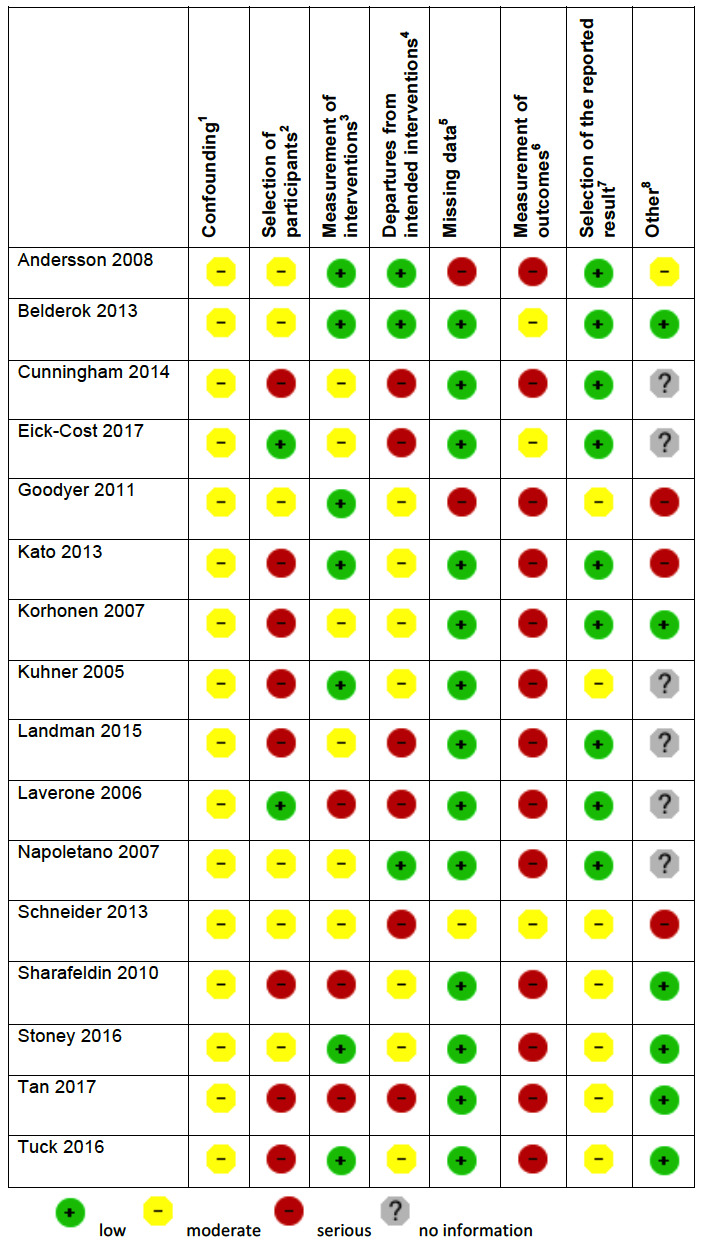
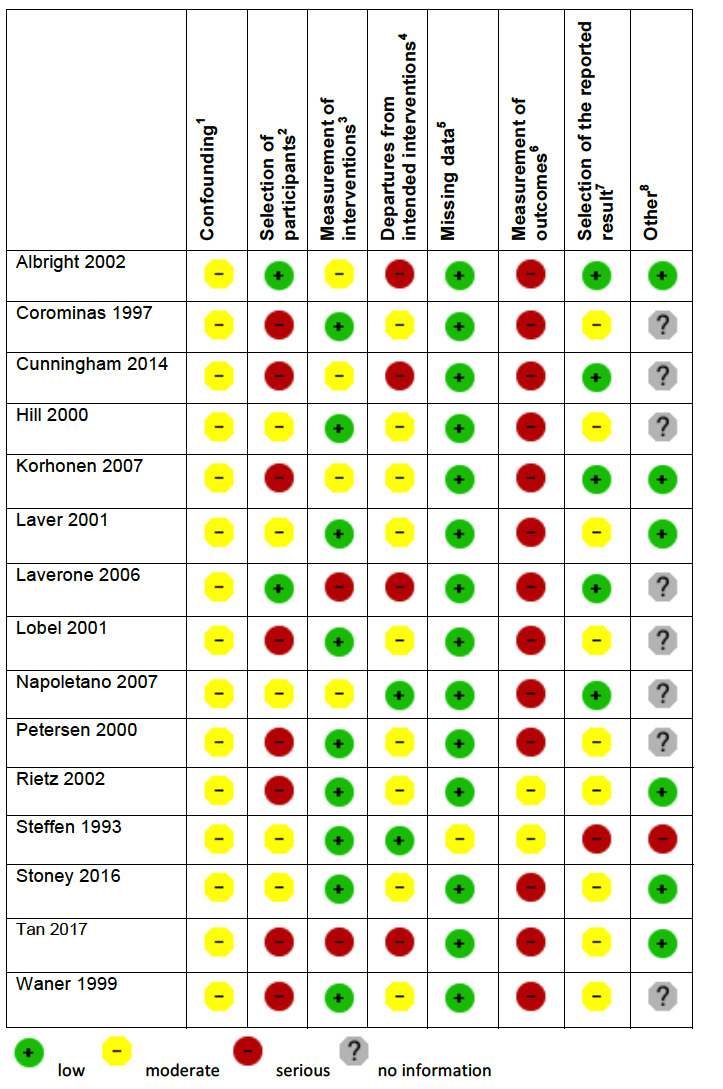
Two review authors independently assessed the eligibility and risk of bias of trials, extracted and analysed data. We compared dichotomous outcomes using risk ratios (RR) with 95% confidence intervals (CI). Prespecified adverse outcomes are included in 'Summary of findings' tables, with the best available estimate of the absolute frequency of each outcome in short-term international travellers. We assessed the certainty of the evidence using the GRADE approach.
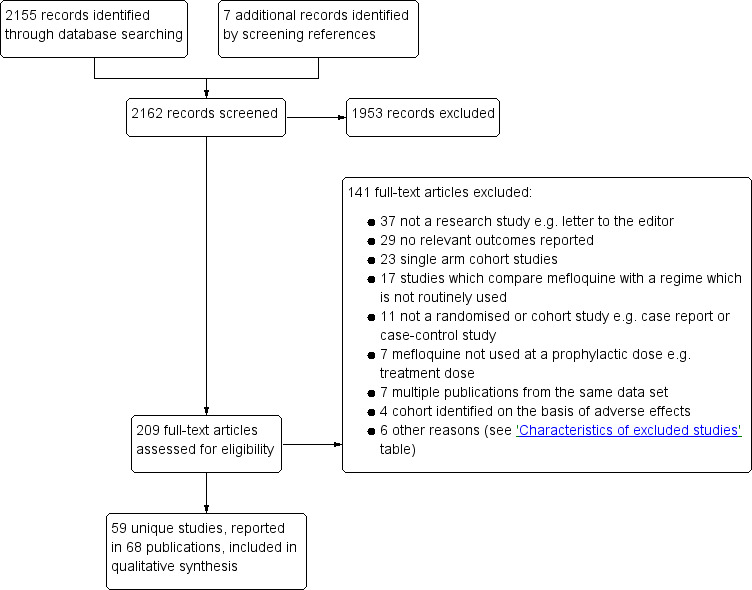
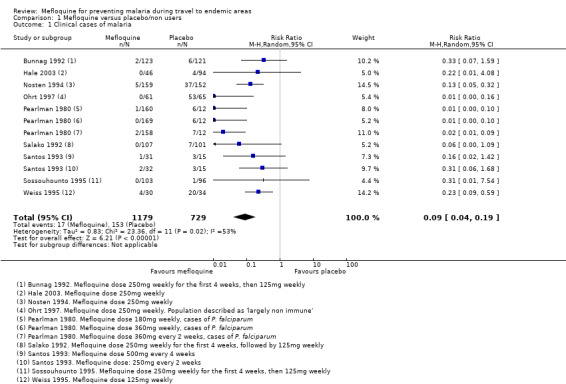
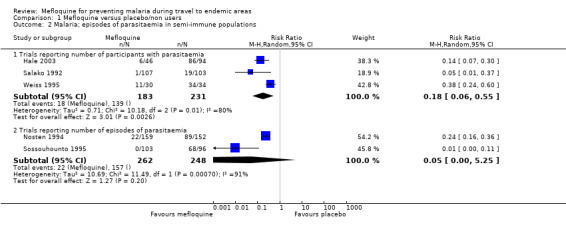
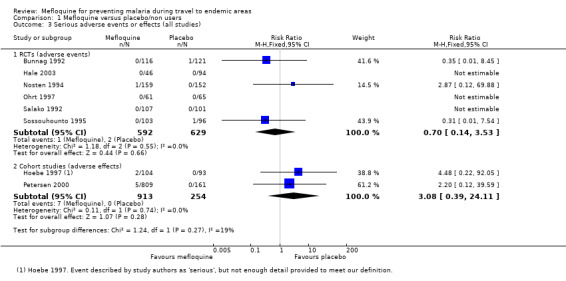
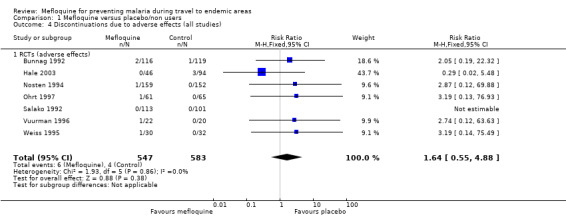
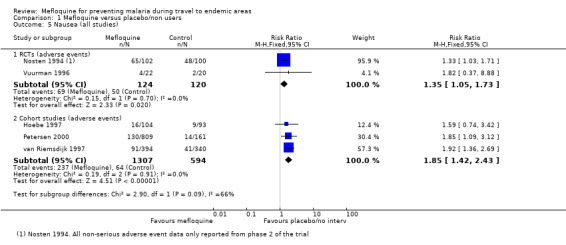
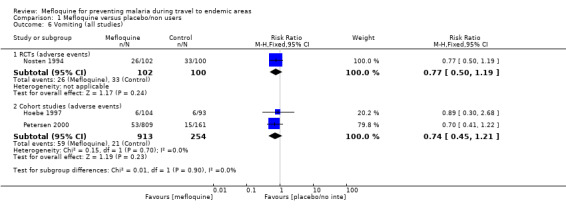
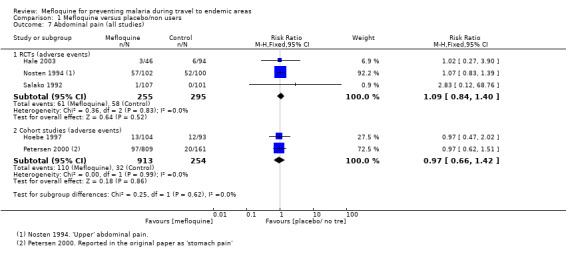
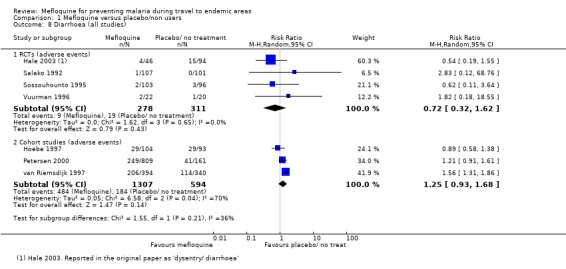
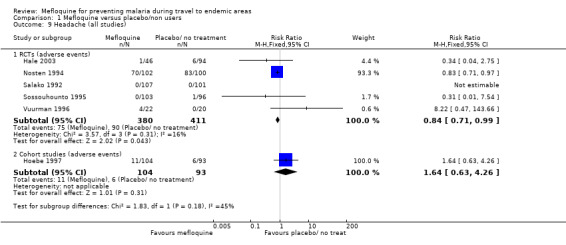
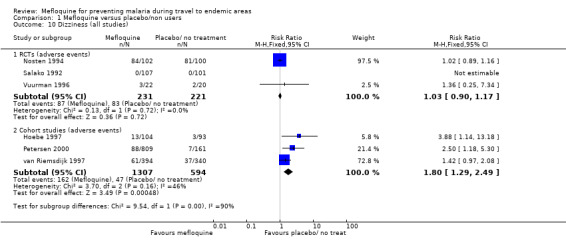
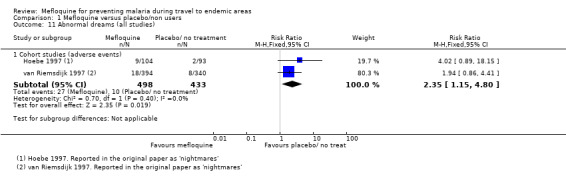
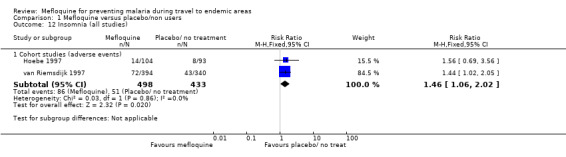
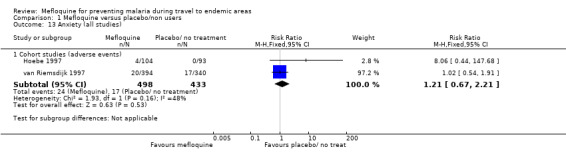
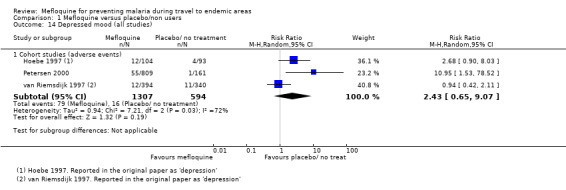
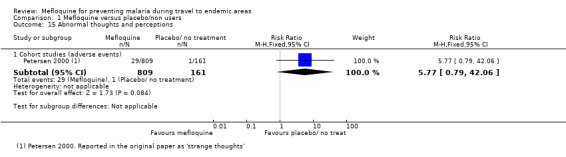
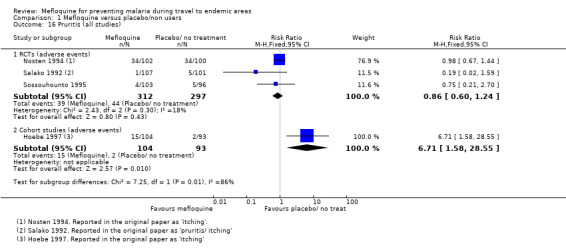
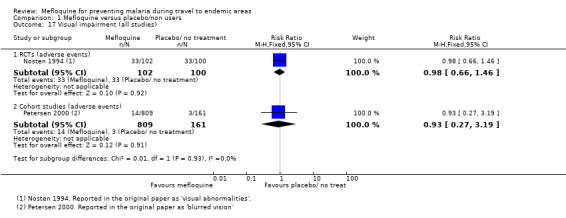
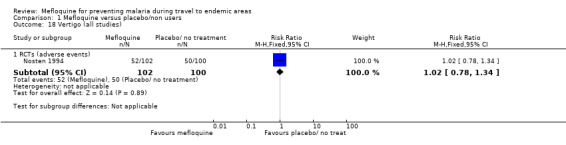
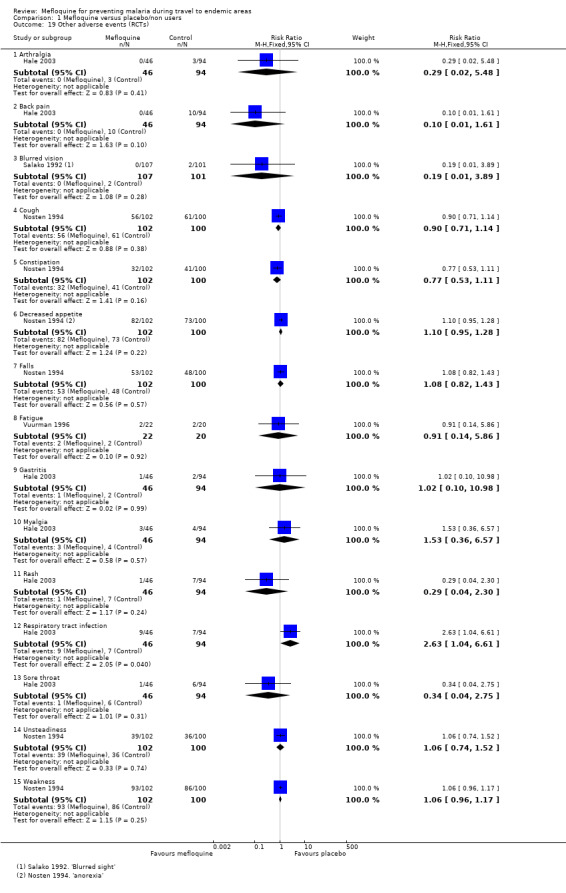
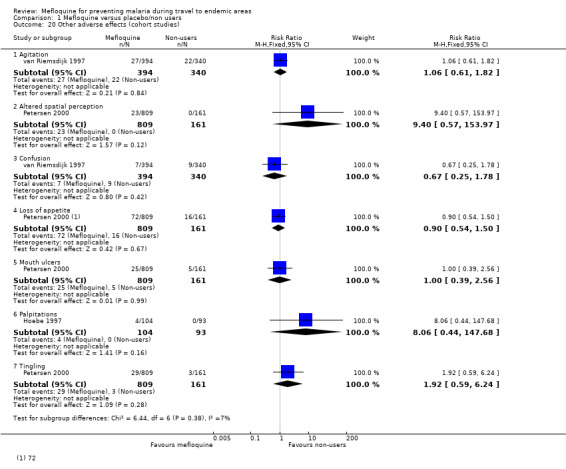
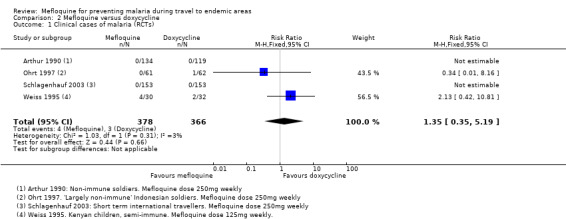
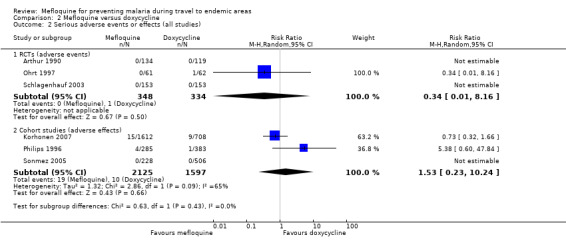
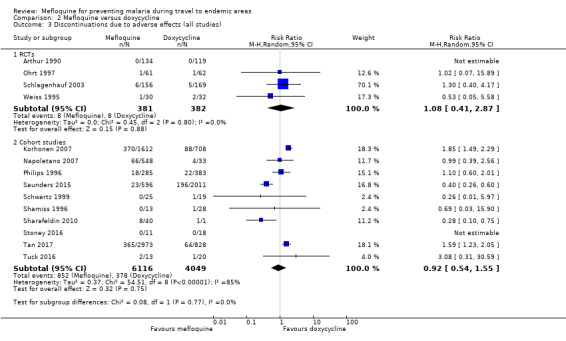
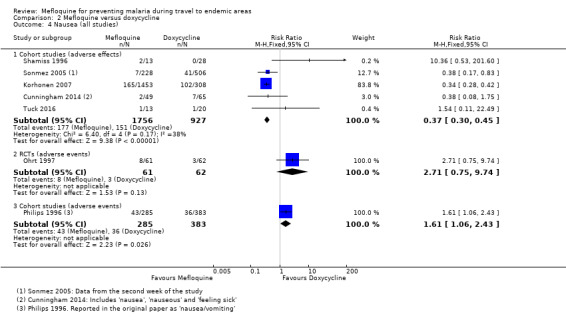
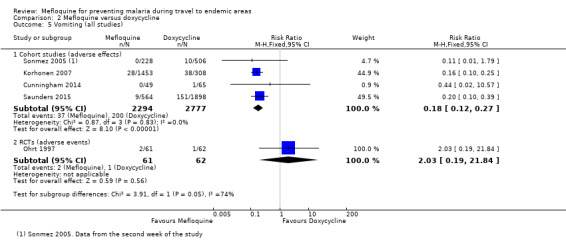
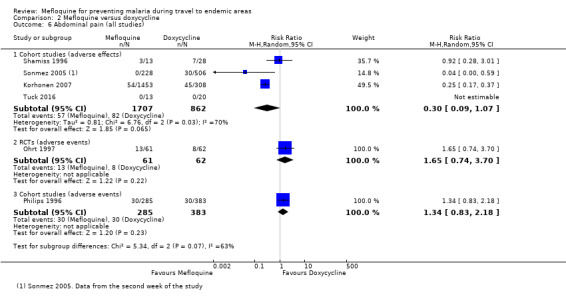
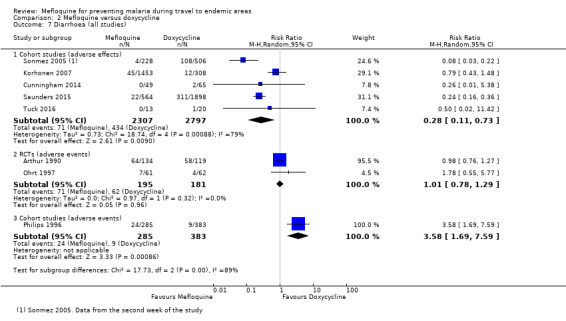
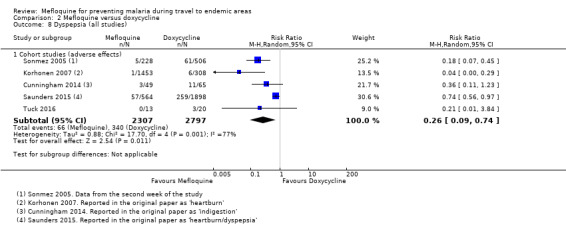
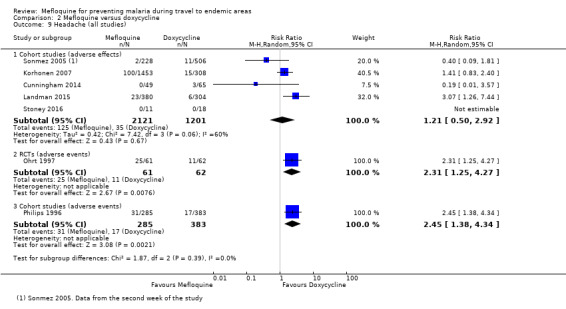
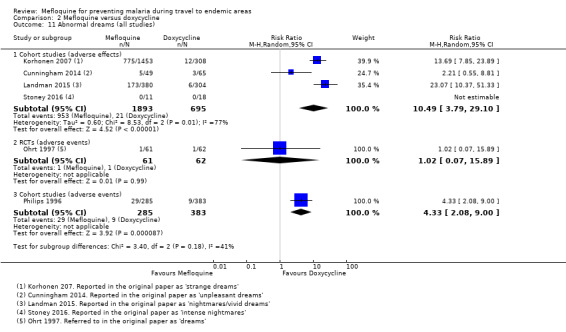
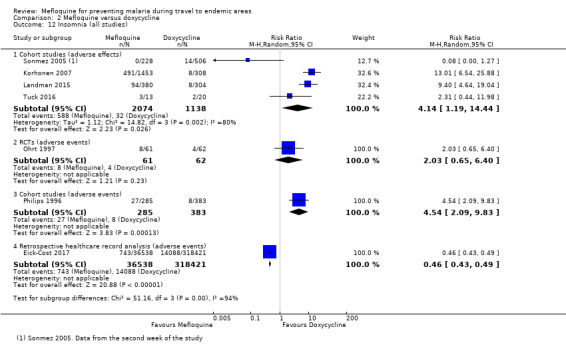
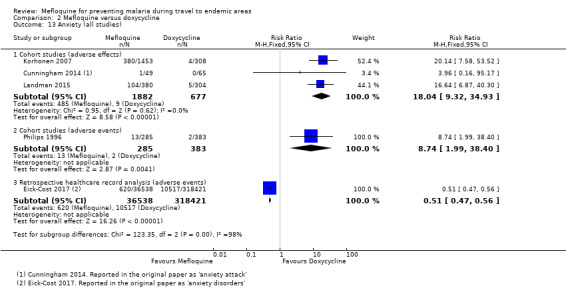
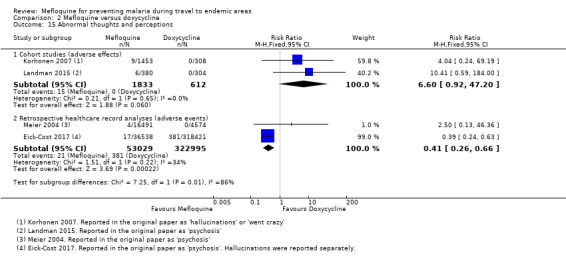
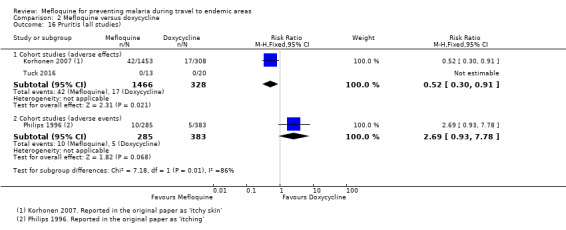
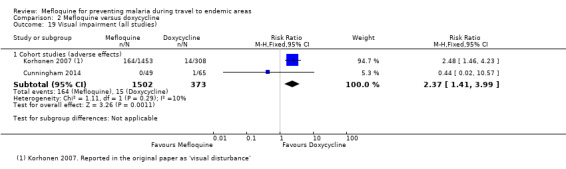
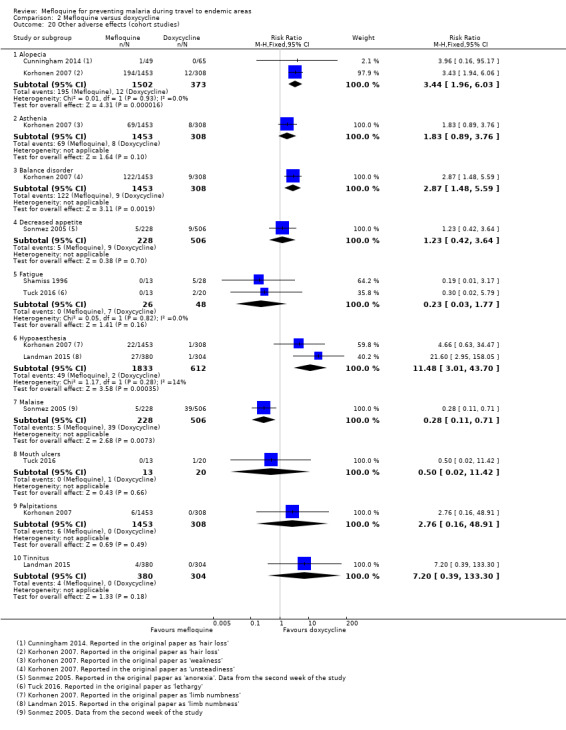
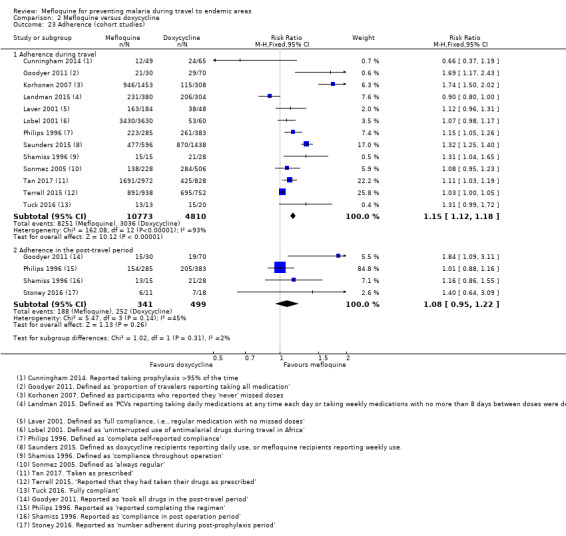
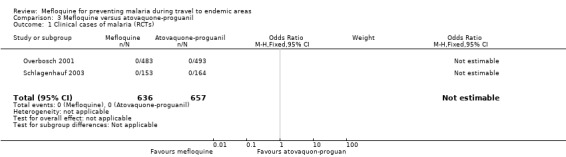
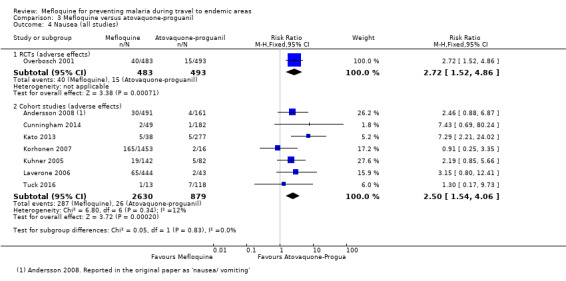
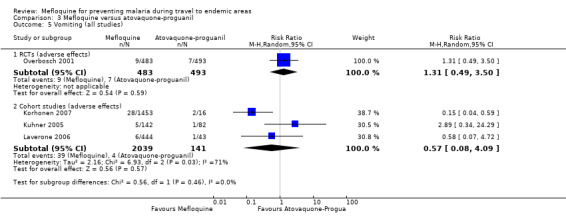
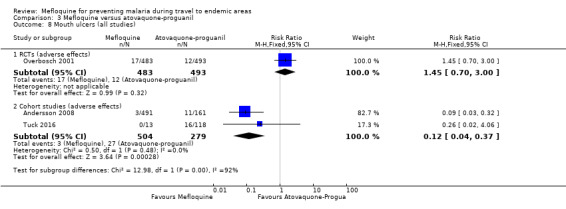
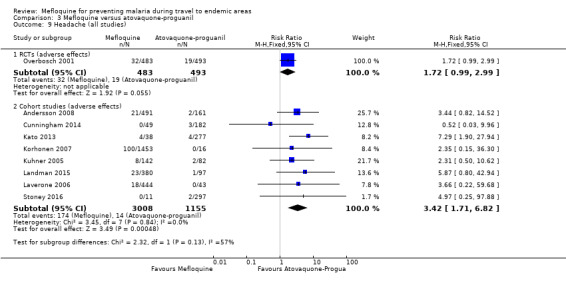
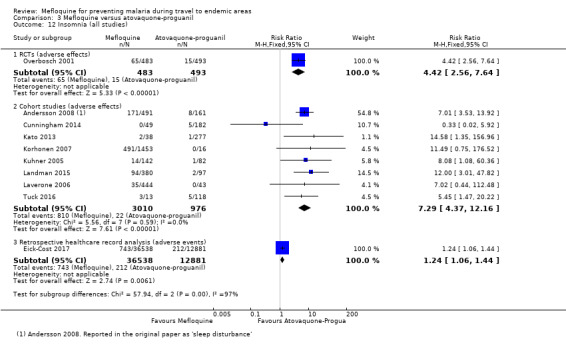
We included 20 RCTs (11,470 participants); 35 cohort studies (198,493 participants); and four large retrospective analyses of health records (800,652 participants). Nine RCTs explicitly excluded participants with a psychiatric history, and 25 cohort studies stated that the choice of antimalarial agent was based on medical history and personal preference. Most RCTs and cohort studies collected data on self-reported or clinician-assessed symptoms, rather than formal medical diagnoses. Mefloquine efficacyOf 12 trials comparing mefloquine and placebo, none were performed in short-term international travellers, and most populations had a degree of immunity to malaria. The percentage of people developing a malaria episode in the control arm varied from 1% to 82% (median 22%) and 0% to 13% in the mefloquine group (median 1%).In four RCTs that directly compared mefloquine, atovaquone-proguanil and doxycycline in non-immune, short-term international travellers, only one clinical case of malaria occurred (4 trials, 1822 participants). Mefloquine safety versus atovaquone-proguanil Participants receiving mefloquine were more likely to discontinue their medication due to adverse effects than atovaquone-proguanil users (RR 2.86, 95% CI 1.53 to 5.31; 3 RCTs, 1438 participants; high-certainty evidence). There were few serious adverse effects reported with mefloquine (15/2651 travellers) and none with atovaquone-proguanil (940 travellers).One RCT and six cohort studies reported on our prespecified adverse effects. In the RCT with short-term travellers, mefloquine users were more likely to report abnormal dreams (RR 2.04, 95% CI 1.37 to 3.04, moderate-certainty evidence), insomnia (RR 4.42, 95% CI 2.56 to 7.64, moderate-certainty evidence), anxiety (RR 6.12, 95% CI 1.82 to 20.66, moderate-certainty evidence), and depressed mood during travel (RR 5.78, 95% CI 1.71 to 19.61, moderate-certainty evidence). The cohort studies in longer-term travellers were consistent with this finding but most had larger effect sizes. Mefloquine users were also more likely to report nausea (high-certainty evidence) and dizziness (high-certainty evidence).Based on the available evidence, our best estimates of absolute effect sizes for mefloquine versus atovaquone-proguanil are 6% versus 2% for discontinuation of the drug, 13% versus 3% for insomnia, 14% versus 7% for abnormal dreams, 6% versus 1% for anxiety, and 6% versus 1% for depressed mood. Mefloquine safety versus doxycyclineNo difference was found in numbers of serious adverse effects with mefloquine and doxycycline (low-certainty evidence) or numbers of discontinuations due to adverse effects (RR 1.08, 95% CI 0.41 to 2.87; 4 RCTs, 763 participants; low-certainty evidence).Six cohort studies in longer-term occupational travellers reported our prespecified adverse effects; one RCT in military personnel and one cohort study in short-term travellers reported adverse events. Mefloquine users were more likely to report abnormal dreams (RR 10.49, 95% CI 3.79 to 29.10; 4 cohort studies, 2588 participants, very low-certainty evidence), insomnia (RR 4.14, 95% CI 1.19 to 14.44; 4 cohort studies, 3212 participants, very low-certainty evidence), anxiety (RR 18.04, 95% CI 9.32 to 34.93; 3 cohort studies, 2559 participants, very low-certainty evidence), and depressed mood (RR 11.43, 95% CI 5.21 to 25.07; 2 cohort studies, 2445 participants, very low-certainty evidence). The findings of the single cohort study reporting adverse events in short-term international travellers were consistent with this finding but the single RCT in military personnel did not demonstrate a difference between groups in frequencies of abnormal dreams or insomnia.Mefloquine users were less likely to report dyspepsia (RR 0.26, 95% CI 0.09 to 0.74; 5 cohort studies, 5104 participants, low certainty-evidence), photosensitivity (RR 0.08, 95% CI 0.05 to 0.11; 2 cohort studies, 1875 participants, very low-certainty evidence), vomiting (RR 0.18, 95% CI 0.12 to 0.27; 4 cohort studies, 5071 participants, very low-certainty evidence), and vaginal thrush (RR 0.10, 95% CI 0.06 to 0.16; 1 cohort study, 1761 participants, very low-certainty evidence).Based on the available evidence, our best estimates of absolute effect for mefloquine versus doxycyline were: 2% versus 2% for discontinuation, 12% versus 3% for insomnia, 31% versus 3% for abnormal dreams, 18% versus 1% for anxiety, 11% versus 1% for depressed mood, 4% versus 14% for dyspepsia, 2% versus 19% for photosensitivity, 1% versus 5% for vomiting, and 2% versus 16% for vaginal thrush.Additional analyses, including comparisons of mefloquine with chloroquine, added no new information. Subgroup analysis by study design, duration of travel, and military versus non-military participants, provided no conclusive findings.
AUTHORS' CONCLUSIONS: The absolute risk of malaria during short-term travel appears low with all three established antimalarial agents (mefloquine, doxycycline, and atovaquone-proguanil).The choice of antimalarial agent depends on how individual travellers assess the importance of specific adverse effects, pill burden, and cost. Some travellers will prefer mefloquine for its once-weekly regimen, but this should be balanced against the increased frequency of abnormal dreams, anxiety, insomnia, and depressed mood.
甲氟喹是常用于预防前往疟疾流行地区旅行者感染疟疾的四种抗疟药物之一。尽管其疗效显著,但关于其心理副作用仍存在争议。
总结甲氟喹用于旅行者疟疾预防的疗效和安全性。
我们检索了Cochrane传染病小组专业注册库;Cochrane图书馆中发表的Cochrane对照试验中心注册库(CENTRAL);MEDLINE;Embase(OVID);TOXLINE(https://toxnet.nlm.nih.gov/newtoxnet/toxline.htm);以及拉丁美洲和加勒比卫生科学数据库(LILACS)。我们还检索了世界卫生组织(WHO)国际临床试验注册平台(ICTRP;http://www.who.int/ictrp/en/)和ClinicalTrials.gov(https://clinicaltrials.gov/ct2/home)以查找正在进行的试验,检索词为“甲氟喹”、“Lariam”和“疟疾”。检索日期为2017年6月22日。
我们纳入了随机对照试验(用于疗效和安全性)和非随机队列研究(用于安全性)。我们将预防性使用甲氟喹与安慰剂、不治疗或另一种推荐的抗疟药物进行比较。我们的研究人群包括所有成年人和儿童,包括孕妇。
两位综述作者独立评估试验的合格性和偏倚风险,提取并分析数据。我们使用风险比(RR)和95%置信区间(CI)比较二分结局。预先设定的不良结局包含在“结果总结”表格中,列出了短期国际旅行者中每种结局的绝对频率的最佳可用估计值。我们使用GRADE方法评估证据的确定性。
我们纳入了20项随机对照试验(11470名参与者);35项队列研究(198493名参与者);以及四项大型健康记录回顾性分析(800652名参与者)。九项随机对照试验明确排除了有精神病史的参与者,25项队列研究表明抗疟药物的选择基于病史和个人偏好。大多数随机对照试验和队列研究收集的是自我报告或临床医生评估的症状数据,而非正式的医学诊断数据。
在比较甲氟喹和安慰剂的12项试验中,没有一项是在短期国际旅行者中进行的,且大多数人群对疟疾有一定程度的免疫力。对照组中出现疟疾发作的人群比例从1%到82%(中位数为22%)不等,甲氟喹组为0%到13%(中位数为1%)。在四项直接比较甲氟喹、阿托伐醌 - 氯胍和多西环素在无免疫力的短期国际旅行者中的随机对照试验中,仅出现了1例疟疾临床病例(4项试验,1822名参与者)。
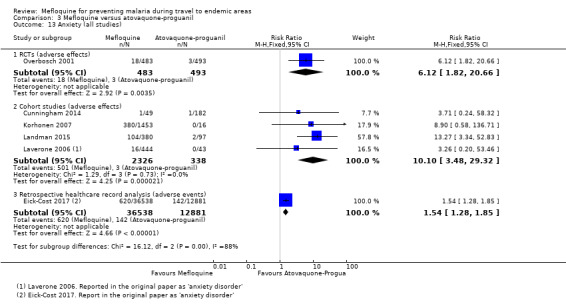
甲氟喹与阿托伐醌 - 氯胍的安全性比较:与使用阿托伐醌 - 氯胍的参与者相比,使用甲氟喹的参与者因不良反应而停药的可能性更高(RR 2.86,95%CI 1.53至5.31;3项随机对照试验,1438名参与者;高确定性证据)。报告的甲氟喹严重不良反应较少(2651名旅行者中有15例),阿托伐醌 - 氯胍则无严重不良反应报告(940名旅行者)。一项随机对照试验和六项队列研究报告了我们预先设定的不良反应。在短期旅行者的随机对照试验中,使用甲氟喹的参与者更有可能报告异常梦境(RR 2.04,95%CI 1.37至3.04,中度确定性证据)、失眠(RR 4.42,95%CI 2.56至7.64,中度确定性证据)、焦虑(RR 6.12,95%CI 1.82至20.66,中度确定性证据)以及旅行期间情绪低落(RR 5.78,95%CI 1.71至19.61,中度确定性证据)。长期旅行者的队列研究结果与此一致,但大多数效应量更大。使用甲氟喹的参与者也更有可能报告恶心(高确定性证据)和头晕(高确定性证据)。基于现有证据,我们对甲氟喹与阿托伐醌 - 氯胍的绝对效应量的最佳估计分别为:停药率6%对2%,失眠率13%对3%,异常梦境率14%对7%,焦虑率6%对1%,情绪低落率6%对1%。
甲氟喹和多西环素的严重不良反应数量无差异(低确定性证据),因不良反应停药的数量也无差异(RR 1.08,95%CI 0.41至2.87;4项随机对照试验,763名参与者;低确定性证据)。六项针对长期职业旅行者的队列研究报告了我们预先设定的不良反应;一项针对军事人员的随机对照试验和一项针对短期旅行者的队列研究报告了不良事件。使用甲氟喹的参与者更有可能报告异常梦境(RR 10.49,95%CI 3.79至29.10;4项队列研究,2588名参与者,极低确定性证据)、失眠(RR 4.14,95%CI 1.19至14.44;4项队列研究,3212名参与者,极低确定性证据)、焦虑(RR 18.04,95%CI 9.32至34.93;3项队列研究,2559名参与者,极低确定性证据)以及情绪低落(RR 11.