Carow Katrin, Read Christina, Häfner Norman, Runnebaum Ingo B, Corner Adam, Dürst Matthias
Klinik und Poliklinik für Frauenheilkunde und Fortpflanzungsmedizin, Universitätsklinikum Jena, Am Klinikum 1, 07747, Jena, Germany.
RainDance Technologies, 749 Middlesex Turnpike, Billerica, MA, 01821, USA.
BMC Res Notes. 2017 Oct 30;10(1):532. doi: 10.1186/s13104-017-2846-8.
Qualitative analyses showed that the presence of HPV mRNA in sentinel lymph nodes of cervical cancer patients with pN0 status is associated with significantly decreased recurrence free survival. To further address the clinical potential of the strategy and to define prognostic threshold levels it is necessary to use a quantitative assay. Here, we compare two methods of quantification: digital PCR and standard quantitative PCR.
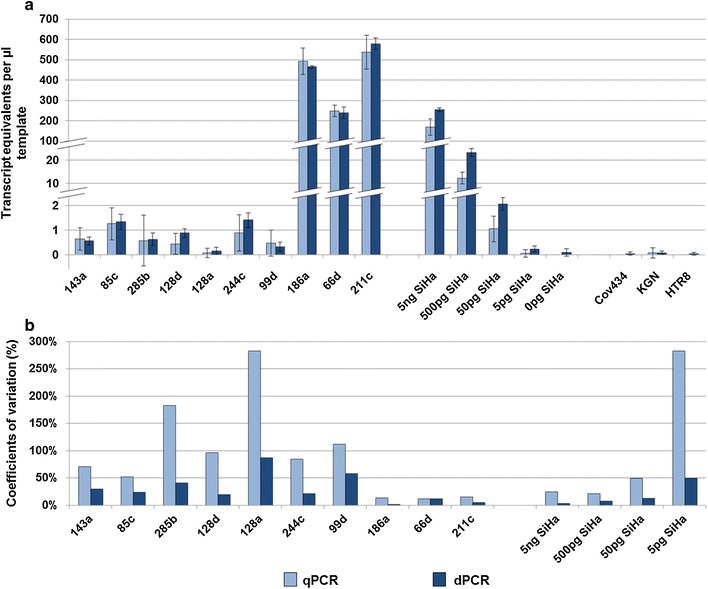
Serial dilutions of 5 ng-5 pg RNA (≙ 500-0.5 cells) of the cervical cancer cell line SiHa were prepared in 5 µg RNA of the HPV-negative human keratinocyte cell line HaCaT. Clinical samples consisted of 10 sentinel lymph nodes with varying HPV transcript levels. Reverse transcription of total RNA (5 µg RNA each) was performed in 100 µl and cDNA aliquots were analyzed by qPCR and dPCR. Digital PCR was run in the RainDrop Digital PCR system (RainDance Technologies) using a probe-based detection of HPV E6/E7 cDNA PCR products with 11 µl template. qPCR was done using a Rotor Gene Q 5plex HRM (Qiagen) amplifying HPV E6/E7 cDNA in a SYBR Green format with 1 µl template.
For the analysis of both, clinical samples and serial dilution samples, dPCR and qPCR showed comparable sensitivity. With regard to reproducibility, both methods differed considerably, especially for low template samples. Here, we found with qPCR a mean variation coefficient of 126% whereas dPCR enabled a significantly lower mean variation coefficient of 40% (p = 0.01). Generally, we saw with dPCR a substantial reduction of subsampling errors, which most likely reflects the large cDNA amounts available for analysis.
Compared to real-time PCR, dPCR shows higher reliability. Thus, our HPV mRNA dPCR assay holds promise for the clinical evaluation of occult tumor cells in histologically tumor-free lymph nodes in future studies.
定性分析表明,在pN0状态的宫颈癌患者前哨淋巴结中HPV mRNA的存在与无复发生存期显著降低相关。为了进一步探讨该策略的临床潜力并确定预后阈值水平,有必要采用定量检测方法。在此,我们比较两种定量方法:数字PCR和标准定量PCR。
在HPV阴性的人角质形成细胞系HaCaT的5μg RNA中制备宫颈癌细胞系SiHa的5ng - 5pg RNA(相当于500 - 0.5个细胞)的系列稀释液。临床样本包括10个HPV转录水平不同的前哨淋巴结。对每个5μg总RNA进行100μl的逆转录,并通过qPCR和dPCR分析cDNA等分试样。数字PCR在RainDrop数字PCR系统(RainDance Technologies)中运行,使用基于探针的方法检测HPV E6/E7 cDNA PCR产物,模板量为11μl。qPCR使用Rotor Gene Q 5plex HRM(Qiagen)以SYBR Green格式扩增HPV E6/E7 cDNA,模板量为1μl。
对于临床样本和系列稀释样本的分析,dPCR和qPCR显示出相当的灵敏度。在重现性方面,两种方法差异很大,尤其是对于低模板样本。在此,我们发现qPCR的平均变异系数为126%,而dPCR的平均变异系数显著更低,为40%(p = 0.01)。总体而言,我们发现dPCR使二次抽样误差大幅降低,这很可能反映了可用于分析的大量cDNA。
与实时PCR相比,dPCR显示出更高的可靠性。因此,我们的HPV mRNA dPCR检测方法有望在未来研究中用于对组织学上无肿瘤的淋巴结中隐匿肿瘤细胞进行临床评估。