Department of Surgery, National University Hospital, Singapore 119074, Singapore.
World J Gastroenterol. 2017 Sep 28;23(36):6741-6746. doi: 10.3748/wjg.v23.i36.6741.
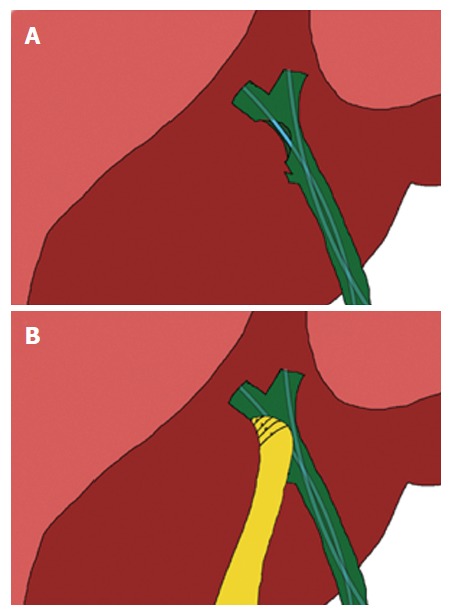
Iatrogenic bile duct injuries during cholecystectomy can present as fulminant intra-abdominal sepsis which precludes immediate repair or biliary reconstruction. We report the case of a 29-year-old female patient who sustained a bile duct injury after an open cholecystectomy in a neighboring country. She presented to our institution 22 d after initial surgery with septic shock and multiple intra-abdominal collections. Endoscopic retrograde cholangiography revealed a large common hepatic duct defect corresponding to a Strasberg type D bile duct injury. Definitive reconstruction such as a hepaticojejunostomy cannot be performed due to the presence of dense adhesions with infected and friable tissues. She underwent a combination of endoscopic biliary stenting and pedicled omental patch repair of the bile duct to control bile leak and sepsis as a bridging procedure to definite hepaticojejunostomy three months later.
在胆囊切除术中引起的医源性胆管损伤可表现为暴发性腹腔内脓毒症,从而妨碍立即进行修复或胆道重建。我们报告了一例 29 岁女性患者的病例,她在邻国行开放性胆囊切除术时发生了胆管损伤。她在初次手术后 22 天因感染性休克和多个腹腔内脓肿就诊于我院。内镜逆行胰胆管造影显示肝总管有一较大的缺损,符合 Strasberg 分型 D 型胆管损伤。由于存在致密粘连和感染性、脆弱组织,无法进行确定性肝肠吻合术。她接受了内镜胆道支架置入和带蒂大网膜补丁修复胆管的联合治疗,以控制胆漏和脓毒症,作为三个月后确定性肝肠吻合术的桥接治疗。