Lee Ryukyung, Ha Heontak, Han Young Seok, Kwon Hyung Jun, Ryeom Hunkyu, Chun Jae Min
Department of Surgery Department of Radiology, Kyungpook National University School of Medicine Daegu, Republic of Korea.
Medicine (Baltimore). 2017 Nov;96(44):e8533. doi: 10.1097/MD.0000000000008533.
Percutaneous transhepatic gallbladder drainage followed by laparoscopic cholecystectomy (PTGBD+LC) is one treatment option for patients with moderate to severe acute cholecystitis (AC). However, the impact of PTGBD on operative difficulties in performing LC is controversial. We designed this retrospective study to clarify the surgical outcomes after PTGBD+LC for the management of patients with moderate to severe AC.The medical records of 85 patients who underwent LC for moderate to severe AC from January 2013 to September 2016 were evaluated. They were divided into 2 groups based on the type of management: group A received PTGBD+LC, and group B received LC without drainage. We compared the patient characteristics, laboratory data which were obtained immediately before surgery or PTGBD at index admission, and surgical outcomes between the 2 groups. We also evaluated possible predictive factors associated with prolonged operative duration after PTGBD+LC.Patients in group A were older and had more comorbidities than those in group B. The laboratory tests obtained at index admission in group A showed higher serum levels of C-reactive protein (CRP) and alkaline phosphatase, and lower albumin levels than those in group B. The surgical outcomes after LC were similar between the 2 groups. However, operative duration was significantly shorter in group A (P = .012). In group A, a higher serum level of CRP was a predictive factor for a prolonged operation (hazard ratio 1.126; 95% confidence interval 1.012-1.253; P = .029). In conclusion, PTGBD+LC can shorten the operative duration in patients with moderate to severe AC, which might improve surgical outcomes in elderly patients with comorbidities, and elevated CRP values predicted a prolonged operation after PTGBD.
经皮经肝胆管胆囊引流术联合腹腔镜胆囊切除术(PTGBD+LC)是中重度急性胆囊炎(AC)患者的一种治疗选择。然而,PTGBD对LC手术难度的影响存在争议。我们设计了这项回顾性研究,以阐明PTGBD+LC治疗中重度AC患者后的手术效果。
对2013年1月至2016年9月因中重度AC接受LC的85例患者的病历进行了评估。根据治疗方式将他们分为两组:A组接受PTGBD+LC,B组接受无引流的LC。我们比较了两组患者的特征、术前或初次入院时PTGBD前即刻获得的实验室数据以及手术结果。我们还评估了与PTGBD+LC后手术时间延长相关的可能预测因素。
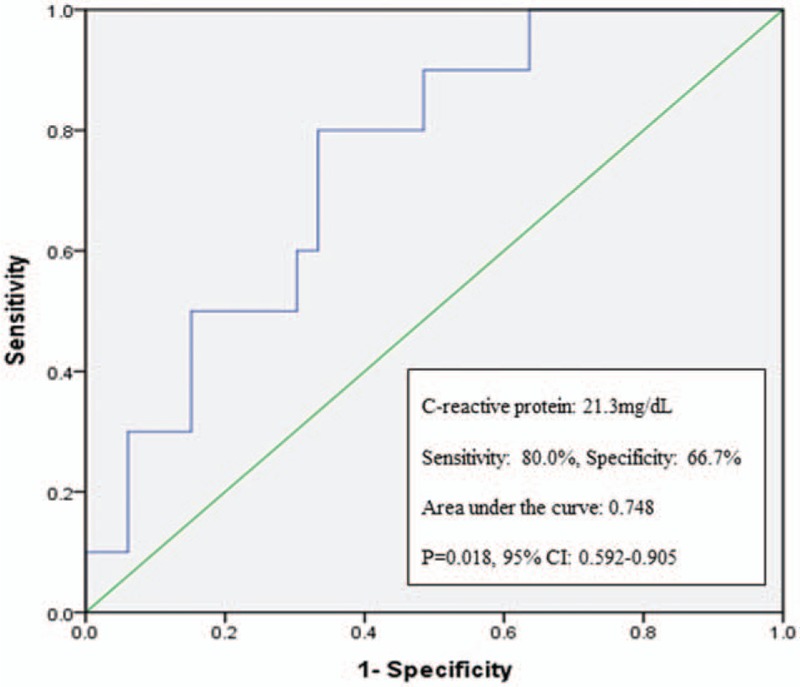
A组患者比B组患者年龄更大,合并症更多。A组初次入院时获得的实验室检查显示,其血清C反应蛋白(CRP)和碱性磷酸酶水平高于B组,白蛋白水平低于B组。两组LC后的手术结果相似。然而,A组的手术时间明显更短(P = 0.012)。在A组中,较高的血清CRP水平是手术时间延长的预测因素(风险比1.126;95%置信区间1.012-1.253;P = 0.029)。
总之,PTGBD+LC可缩短中重度AC患者的手术时间,这可能改善合并症老年患者的手术结果,且CRP值升高预示PTGBD后手术时间延长。