Department of Medicine and Surgery, Plastic Surgery Division, University of Parma, Parma, Italy.
Cutaneous, Mini-Invasive, Regenerative and Plastic Surgery Unit, Parma University Hospital, Parma, Italy.
Biomed Res Int. 2017;2017:6486859. doi: 10.1155/2017/6486859. Epub 2017 Oct 2.
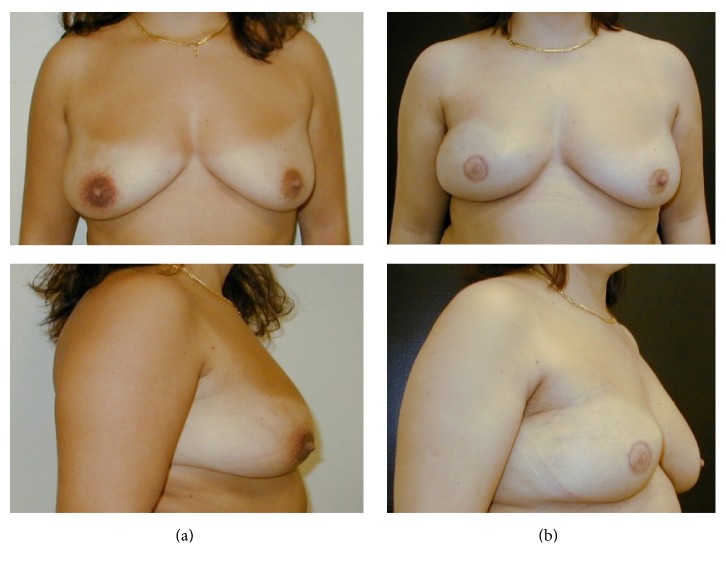
One-stage direct-to-implant immediate breast reconstruction (IBR) is performed simultaneously with breast cancer resection. We explored indications, techniques, and outcomes of IBR to determine its feasibility, safety, and effectiveness.
We reviewed the available literature on one-stage direct-to-implant IBR, with or without acellular dermal matrix (ADM), synthetic mesh, or autologous fat grafting. We analyzed the indications, preoperative work-up, surgical technique, postoperative care, outcomes, and complications.
IBR is indicated for small-to-medium nonptotic breasts and contraindicated in patients who require or have undergone radiotherapy, due to unacceptably high complications rates. Only patients with thick, well-vascularized mastectomy flaps are IBR candidates. Expandable implants should be used for ptotic breasts, while anatomical shaped implants should be used to reconstruct small-to-medium nonptotic breasts. ADMs can be used to cover the implant during IBR and avoid muscle elevation, thereby minimizing postoperative pain. Flap necrosis, reoperation, and implant loss are more common with IBR than conventional two-staged reconstruction, but IBR has advantages such as lack of secondary surgery, faster recovery, and better quality of life.
IBR has good outcomes and patient-satisfaction rates. With ADM use, a shift from conventional reconstruction to IBR has occurred. Drawbacks of IBR can be overcome by careful patient selection.
一期直接植入即刻乳房重建(IBR)与乳腺癌切除术同时进行。我们探讨了 IBR 的适应证、技术和结果,以确定其可行性、安全性和有效性。
我们回顾了关于一期直接植入 IBR 的文献,包括使用或不使用脱细胞真皮基质(ADM)、合成网或自体脂肪移植的情况。我们分析了适应证、术前检查、手术技术、术后护理、结果和并发症。
IBR 适用于小至中等非下垂乳房,不适用于需要或已接受放疗的患者,因为并发症发生率高且不可接受。只有厚而血供良好的乳房切除术皮瓣患者才是 IBR 的候选者。对于下垂乳房,应使用可扩张植入物,而对于小至中等非下垂乳房,应使用解剖形状的植入物进行重建。ADM 可用于在 IBR 期间覆盖植入物,避免肌肉抬高,从而最大限度地减少术后疼痛。与传统的两阶段重建相比,IBR 更常见的是皮瓣坏死、再次手术和植入物丢失,但 IBR 具有无需二次手术、恢复更快和生活质量更好等优点。
IBR 具有良好的结果和患者满意度。随着 ADM 的使用,从传统重建向 IBR 的转变已经发生。通过仔细选择患者,可以克服 IBR 的缺点。