Iba Toshiaki, Hagiwara Akiyoshi, Saitoh Daizoh, Anan Hideaki, Ueki Yutaka, Sato Koichi, Gando Satoshi
Department of Emergency and Disaster Medicine, Juntendo University Graduate School of Medicine, 2-1-1 Hongo Bunkyo-ku, Tokyo, 113-8421, Japan.
National Center for Global Health and Medicine, Emergency Medicine and Critical Care, Tokyo, Japan.
Ann Intensive Care. 2017 Nov 2;7(1):110. doi: 10.1186/s13613-017-0332-z.
No single anticoagulant has been proven effective for sepsis-associated disseminated intravascular coagulation (DIC). Thus, the concomitant use of antithrombin concentrate and recombinant thrombomodulin has been conceived. This observational study was conducted to investigate the efficacy and safety of this combination therapy.
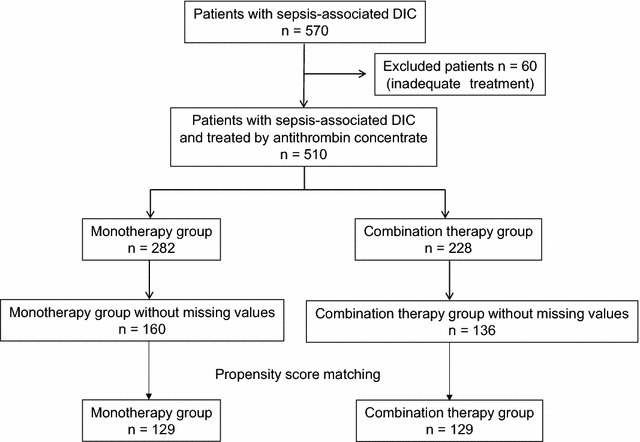
A total of 510 septic DIC patients who received antithrombin substitution were retrospectively analyzed. Among them, 228 were treated with antithrombin and recombinant thrombomodulin (combination therapy) and the rest were treated with antithrombin alone (monotherapy). Propensity score matching created 129 matched pairs, and 28-day all-cause mortality, DIC scores, the sequential organ failure assessment (SOFA) scores, and the incidence of bleeding were compared.
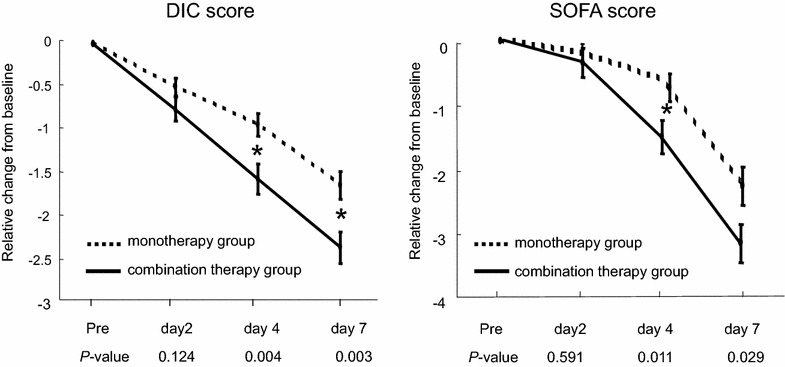
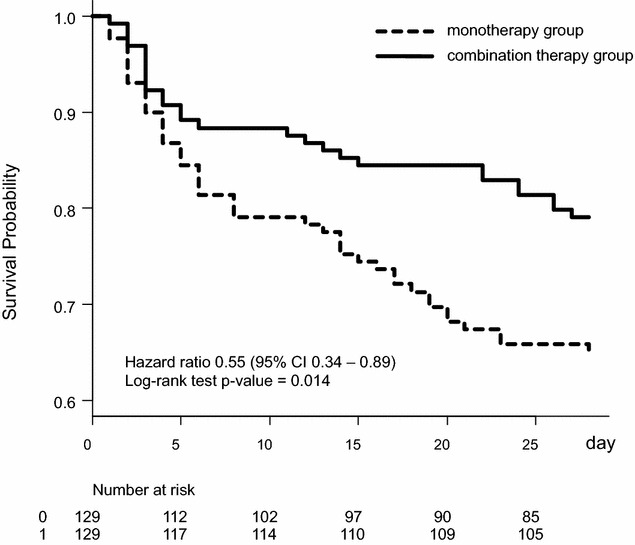
A log-rank test revealed a significant association between combination therapy and a lower 28-day mortality rate (hazard ratio 0.49, 95% confidence interval 0.29-0.82, P = 0.006) in the matched pairs. The DIC scores and the SOFA scores in the combination therapy group were significantly lower than those in the monotherapy group on Day 4 and Day 7. The incidence of bleeding did not differ between the groups (2.11 vs. 2.31%, P = 1.000).
The current study demonstrated the potential benefit of adding recombinant thrombomodulin to antithrombin. The co-administration of these two anticoagulants was associated with reduced mortality among patients with sepsis-induced DIC without increasing the risk of bleeding.
尚无单一抗凝剂被证明对脓毒症相关的弥散性血管内凝血(DIC)有效。因此,有人设想同时使用抗凝血酶浓缩物和重组血栓调节蛋白。本观察性研究旨在调查这种联合治疗的疗效和安全性。
对总共510例接受抗凝血酶替代治疗的脓毒症DIC患者进行回顾性分析。其中,228例接受抗凝血酶和重组血栓调节蛋白治疗(联合治疗),其余患者仅接受抗凝血酶治疗(单一治疗)。倾向评分匹配产生了129对匹配对,并比较了28天全因死亡率、DIC评分、序贯器官衰竭评估(SOFA)评分和出血发生率。
对数秩检验显示,在匹配对中,联合治疗与较低的28天死亡率显著相关(风险比0.49,95%置信区间0.29 - 0.82,P = 0.006)。联合治疗组在第4天和第7天的DIC评分和SOFA评分显著低于单一治疗组。两组之间的出血发生率没有差异(2.11%对2.31%,P = 1.000)。
当前研究证明了在抗凝血酶基础上加用重组血栓调节蛋白的潜在益处。这两种抗凝剂的联合使用与脓毒症诱导的DIC患者死亡率降低相关,且不增加出血风险。