Department of Clinical Oncology, Tuen Mun Hospital, Hong Kong, Hong Kong.
Department of Non-Communicable Disease Epidemiology, Cancer Survival Group, London School of Hygiene & Tropical Medicine, London, UK.
BMJ Open. 2017 Nov 3;7(11):e017904. doi: 10.1136/bmjopen-2017-017904.
The clinical course and prognosis of follicular lymphoma (FL) are diverse and associated with the patient's immune response. We investigated the lymphocyte-to-monocyte ratio (LMR) and neutrophil-to-lymphocyte ratio (NLR) as prognostic factors in patients with FL, including those receiving radiotherapy.
A retrospective cohort study.
Regional cancer centre in Hong Kong.
88 patients with histologically proven FL diagnosed between 2000 and 2014.
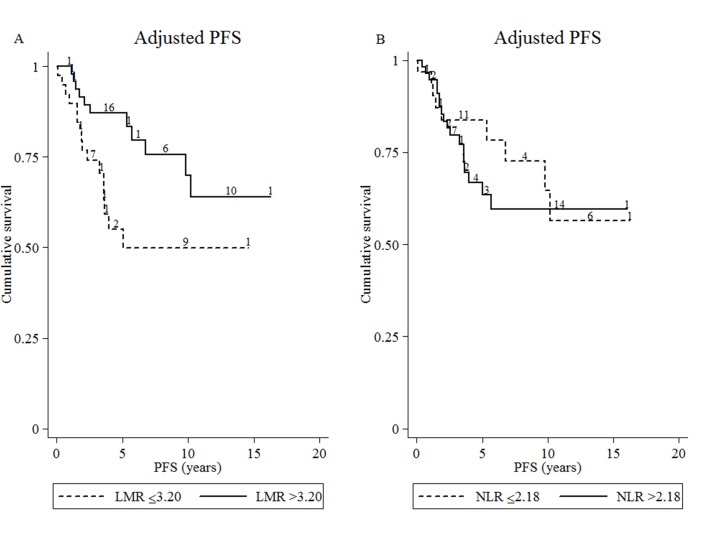
The best LMR and NLR cut-off values were determined using cross-validated areas under the receiver operating characteristic curves. The extent to which progression-free survival (PFS) and overall survival differed by NLR and LMR cut-off values was assessed using Kaplan-Meier analysis and log-rank tests. A Cox proportional hazards model was fitted to adjust for confounders.
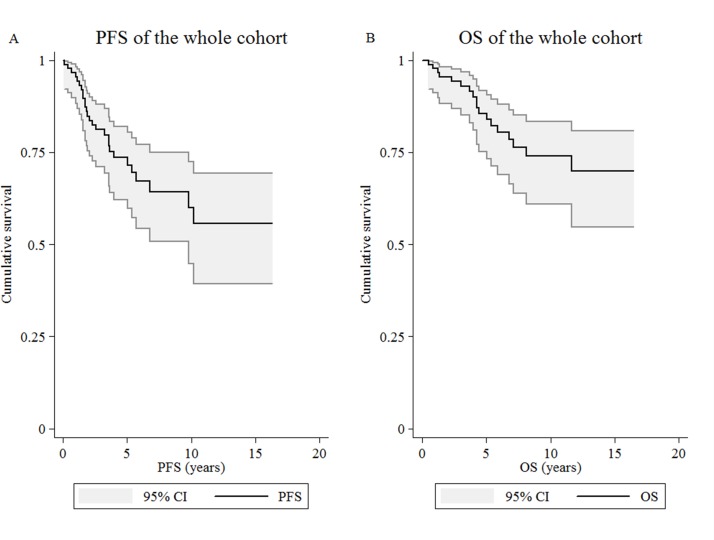
The best cut-off values for LMR and NLR were 3.20 and 2.18, respectively. The 5-year PFS was 73.6%. After multivariate adjustment, high LMR (>3.20) at diagnosis was associated with superior PFS, with a HR of 0.31 (95% CI 0.13 to 0.71), whereas high NLR at relapse was associated with poorer postprogression survival (HR 1.24, 95% CI 1.04 to 1.49).
Baseline LMR and NLR at relapse were shown to be independent prognostic factors in FL. LMR and NLR are cheap and widely available biomarkers that could be used in combination with the Follicular Lymphoma International Prognostic Index by clinicians to better predict prognosis.
滤泡性淋巴瘤(FL)的临床病程和预后各不相同,与患者的免疫反应有关。我们研究了淋巴细胞与单核细胞比值(LMR)和中性粒细胞与淋巴细胞比值(NLR)作为 FL 患者的预后因素,包括接受放疗的患者。
回顾性队列研究。
中国香港地区癌症中心。
88 例 2000 年至 2014 年间经组织学证实的滤泡性淋巴瘤患者。
使用交叉验证的受试者工作特征曲线下面积确定最佳 LMR 和 NLR 截断值。使用 Kaplan-Meier 分析和对数秩检验评估 NLR 和 LMR 截断值对无进展生存期(PFS)和总生存期的影响。使用 Cox 比例风险模型进行调整以校正混杂因素。
LMR 和 NLR 的最佳截断值分别为 3.20 和 2.18。5 年 PFS 为 73.6%。经过多变量调整,诊断时高 LMR(>3.20)与较好的 PFS 相关,HR 为 0.31(95%CI 0.13 至 0.71),而复发时高 NLR 与较差的进展后生存相关(HR 1.24,95%CI 1.04 至 1.49)。
基线 LMR 和 NLR 在复发时被证明是 FL 的独立预后因素。LMR 和 NLR 是廉价且广泛可用的生物标志物,可与滤泡性淋巴瘤国际预后指数(FLIPI)结合使用,由临床医生更好地预测预后。