University of Zimbabwe Clinical Research Centre, Harare, Zimbabwe.
MRC Clinical Trials Unit at University College London, London, UK.
Lancet Infect Dis. 2018 Jan;18(1):47-57. doi: 10.1016/S1473-3099(17)30630-8. Epub 2017 Nov 3.
Millions of HIV-infected people worldwide receive antiretroviral therapy (ART) in programmes using WHO-recommended standardised regimens. Recent WHO guidelines recommend a boosted protease inhibitor plus raltegravir as an alternative second-line combination. We assessed whether this treatment option offers any advantage over the standard protease inhibitor plus two nucleoside reverse-transcriptase inhibitors (NRTIs) second-line combination after 144 weeks of follow-up in typical programme settings.
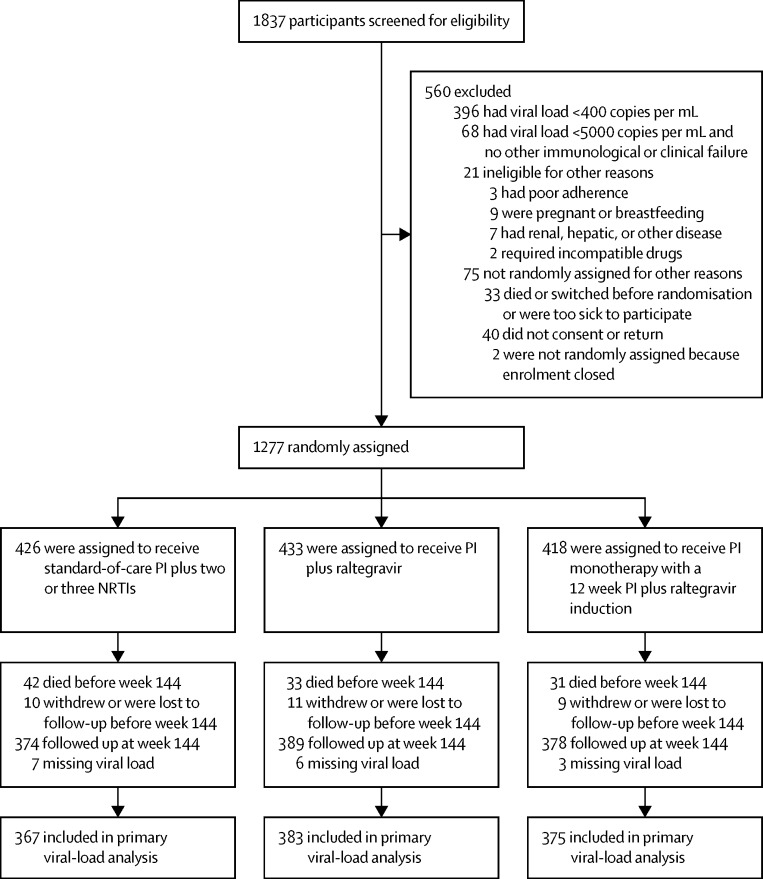
We analysed the 144-week outcomes at the completion of the EARNEST trial, a randomised controlled trial done in HIV-infected adults or adolescents in 14 sites in five sub-Saharan African countries (Uganda, Zimbabwe, Malawi, Kenya, Zambia). Participants were those who were no longer responding to non-NRTI-based first-line ART, as assessed with WHO criteria, confirmed by viral-load testing. Participants were randomly assigned to receive a ritonavir-boosted protease inhibitor (lopinavir 400 mg with ritonavir 100 mg, twice per day) plus two or three clinician-selected NRTIs (protease inhibitor plus NRTI group), protease inhibitor plus raltegravir (400 mg twice per day; protease inhibitor plus raltegravir group), or protease inhibitor monotherapy (plus raltegravir induction for first 12 weeks, re-intensified to combination therapy after week 96; protease inhibitor monotherapy group). Randomisation was by computer-generated randomisation sequence, with variable block size. The primary outcome was viral load of less than 400 copies per mL at week 144, for which we assessed non-inferiority with a one-sided α of 0·025, and superiority with a two-sided α of 0·025. The EARNEST trial is registered with ISRCTN, number 37737787.
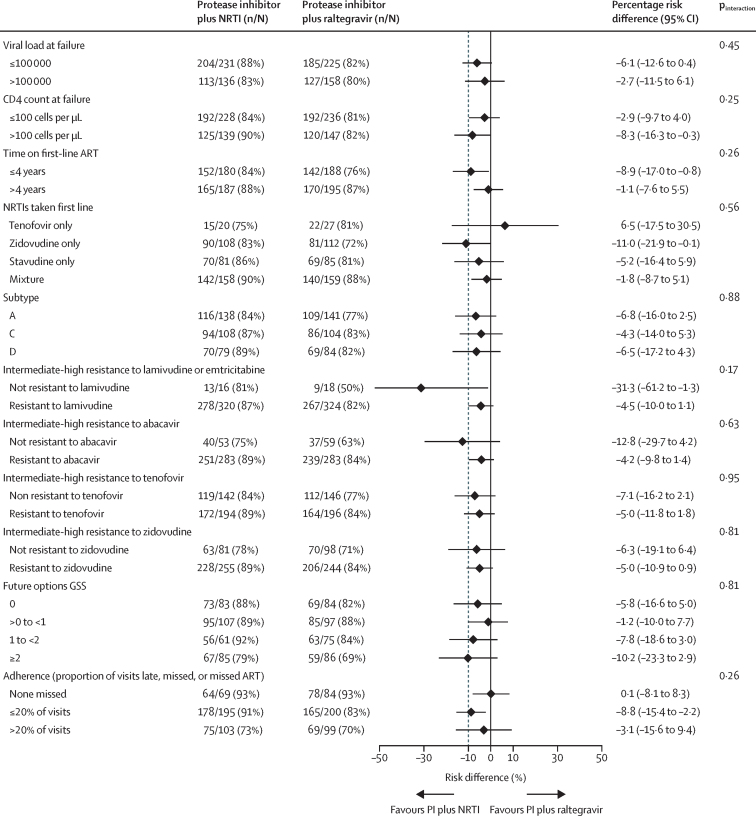
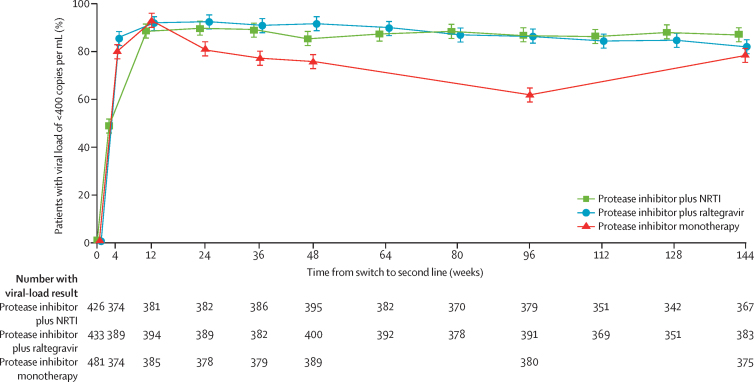
Between April 12, 2010, and April 29, 2011, 1837 patients were screened for eligibility, of whom 1277 patients were randomly assigned to an intervention group. In the primary (complete-case) analysis at 144 weeks, 317 (86%) of 367 in the protease inhibitor plus NRTI group had viral loads of less than 400 copies per mL compared with 312 (81%) of 383 in the protease inhibitor plus raltegravir group (p=0·07; lower 95% confidence limit for difference 10·2% vs specified non-inferiority margin 10%). In the protease inhibitor monotherapy group, 292 (78%) of 375 had viral loads of less than 400 copies per mL; p=0·003 versus the protease inhibitor plus NRTI group at 144 weeks. There was no difference between groups in serious adverse events, grade 3 or 4 adverse events (total or ART-related), or events that resulted in treatment modification.
Protease inhibitor plus raltegravir offered no advantage over protease inhibitor plus NRTI in virological efficacy or safety. In the primary analysis, protease inhibitor plus raltegravir did not meet non-inferiority criteria. A regimen of protease inhibitor with NRTIs remains the best standardised second-line regimen for use in programmes in resource-limited settings.
European and Developing Countries Clinical Trials Partnership (EDCTP), UK Medical Research Council, Instituto de Salud Carlos III, Irish Aid, Swedish International Development Cooperation Agency, Instituto Superiore di Sanita, Merck, ViiV Healthcare, WHO.
全球数以百万计的 HIV 感染者在采用世卫组织推荐的标准化方案的抗逆转录病毒治疗(ART)项目中接受治疗。最近的世卫组织指南建议使用强化蛋白酶抑制剂加雷特格韦作为替代二线联合治疗方案。我们评估了在典型方案环境中,在随访 144 周后,与标准蛋白酶抑制剂加两种核苷逆转录酶抑制剂(NRTIs)二线联合治疗相比,这种治疗选择是否具有任何优势。
我们分析了 EARNEST 试验的 144 周结果,该试验是在五个撒哈拉以南非洲国家(乌干达、津巴布韦、马拉维、肯尼亚、赞比亚)的 14 个地点进行的 HIV 感染成人或青少年的随机对照试验。参与者是那些根据世卫组织标准评估不再对非 NRTI 为基础的一线 ART 有反应的人,通过病毒载量检测得到证实。参与者被随机分配接受利托那韦强化蛋白酶抑制剂(洛匹那韦 400mg 与利托那韦 100mg,每日两次)加两种或三种临床医生选择的 NRTIs(蛋白酶抑制剂加 NRTI 组)、蛋白酶抑制剂加雷特格韦(每日两次 400mg;蛋白酶抑制剂加雷特格韦组)或蛋白酶抑制剂单药治疗(前 12 周加雷特格韦诱导治疗,第 96 周后重新强化为联合治疗;蛋白酶抑制剂单药治疗组)。随机化是通过计算机生成的随机化序列进行的,具有可变的块大小。主要结局是在第 144 周时病毒载量小于 400 拷贝/ml,我们使用单侧 α 值为 0.025 评估非劣效性,使用双侧 α 值为 0.025 评估优越性。EARNEST 试验在 ISRCTN 注册,编号为 37737787。
2010 年 4 月 12 日至 2011 年 4 月 29 日,共有 1837 名患者接受了资格筛选,其中 1277 名患者被随机分配到干预组。在第 144 周的主要(完全病例)分析中,蛋白酶抑制剂加 NRTI 组的 317 名(86%)患者病毒载量小于 400 拷贝/ml,而蛋白酶抑制剂加雷特格韦组的 312 名(81%)患者病毒载量小于 400 拷贝/ml(p=0.07;差异的置信下限下限为 10.2%,低于指定的非劣效性边界 10%)。在蛋白酶抑制剂单药治疗组中,375 名患者中有 292 名(78%)病毒载量小于 400 拷贝/ml;与蛋白酶抑制剂加 NRTI 组相比,p=0.003,在第 144 周。各组之间严重不良事件、3 级或 4 级不良事件(总或与 ART 相关)或导致治疗改变的事件无差异。
蛋白酶抑制剂加雷特格韦在病毒学疗效和安全性方面与蛋白酶抑制剂加 NRTI 相比没有优势。在主要分析中,蛋白酶抑制剂加雷特格韦不符合非劣效性标准。蛋白酶抑制剂加 NRTIs 的方案仍然是资源有限环境中使用的最佳标准化二线方案。
欧洲和发展中国家临床试验伙伴关系(EDCTP)、英国医学研究理事会、西班牙卡洛斯三世卫生研究所、爱尔兰援助署、瑞典国际发展合作署、意大利卫生研究所、默克公司、ViiV 医疗保健公司、世卫组织。