Chandrasekharan P, Rawat M, Reynolds A M, Phillips K, Lakshminrusimha S
Division of Neonatology, Department of Pediatrics, UBMD, Women and Children's Hospital of Buffalo, John R. Oishei Children's Hospital, Buffalo, NY, USA.
Kaleida Health, Women and Children's Hospital of Buffalo, John R. Oishei Children's Hospital, Buffalo, NY, USA.
J Perinatol. 2018 Jan;38(1):86-91. doi: 10.1038/jp.2017.174. Epub 2017 Nov 9.
To study the impact of implementing a protocol to standardize the duration of observation in preterm infants with apnea/bradycardia/desaturation spells before hospital discharge on length of stay (LOS) and readmission rates.
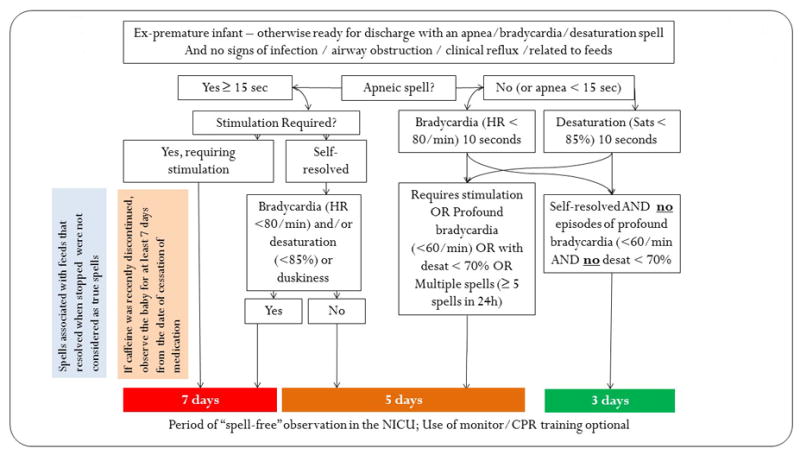
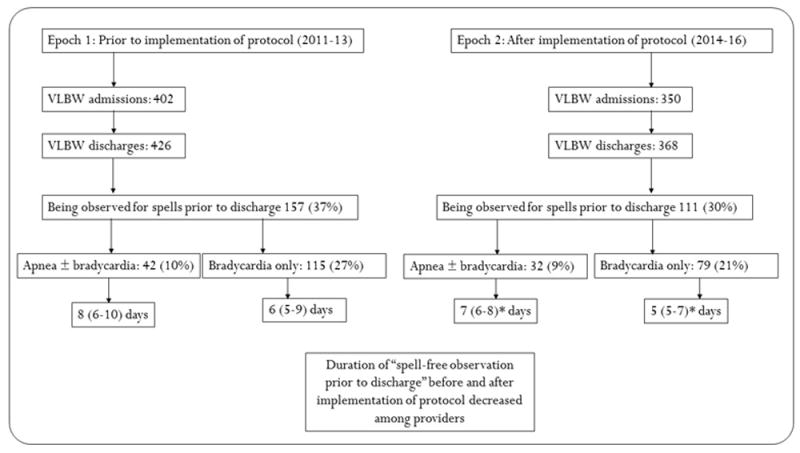
A protocol to standardize the duration of in-hospital observation for preterm infants with apnea, bradycardia and desaturation spells who were otherwise ready for discharge was implemented in December 2013. We evaluated the impact of this protocol on the LOS and readmission rates of very low birth weight infants (VLBW). Data on readmission for apnea and an apparent life-threatening event (ALTE) within 30 days of discharge were collected. The pre-implementation epoch (2011 to 2013) was compared to the post-implementation period (2014 to 2016).
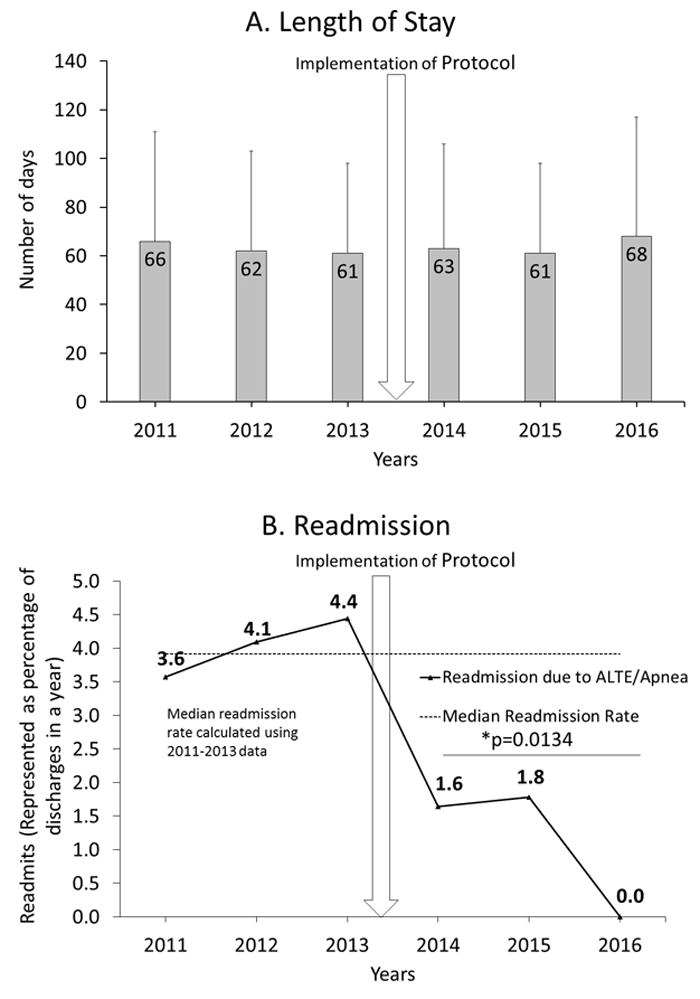
There were 426 and 368 VLBW discharges before and after initiation of the protocol during 2011 to 2013 and 2014 to 2016, respectively. The LOS did not change with protocol implementation (66±42 vs 64±42 days before and after implementation of the protocol, respectively). Interprovider variability on the duration of observation for apneic spells (F-8.8, P=0.04) and bradycardia spells (F-17.4, P<0.001) decreased after implementation of the protocol. The readmission rate for apnea/ALTE after the protocol decreased from 12.1 to 3.4% (P=0.01).
Implementing an institutional protocol for VLBW infants to determine the duration of apnea/bradycardia/ desaturation spell-free observation period as recommended by the American Academy of Pediatrics clinical report did not prolong the LOS but effectively reduced interprovider variability and readmission rates.
研究实施一项方案以规范早产儿呼吸暂停/心动过缓/血氧饱和度下降发作在出院前的观察时长对住院时间(LOS)和再入院率的影响。
2013年12月实施了一项方案,用于规范那些原本已准备好出院但患有呼吸暂停、心动过缓及血氧饱和度下降发作的早产儿的住院观察时长。我们评估了该方案对极低出生体重儿(VLBW)的住院时间和再入院率的影响。收集了出院后30天内因呼吸暂停和明显危及生命事件(ALTE)而再入院的数据。将实施该方案前的时期(2011年至2013年)与实施后的时期(2014年至2016年)进行比较。
在2011年至2013年及2014年至2016年期间,方案启动前和启动后分别有426例和368例VLBW患儿出院。实施该方案后住院时间未发生变化(实施方案前后分别为66±42天和64±42天)。实施该方案后,不同医护人员对呼吸暂停发作观察时长的变异性(F = 8.8,P = 0.04)以及对心动过缓发作观察时长的变异性(F = 17.4,P < 0.001)均有所降低。方案实施后,呼吸暂停/ALTE的再入院率从12.1%降至3.4%(P = 0.01)。
按照美国儿科学会临床报告的建议,为VLBW婴儿实施一项机构方案来确定无呼吸暂停/心动过缓/血氧饱和度下降发作的观察期时长,并未延长住院时间,但有效降低了医护人员之间的变异性和再入院率。