David O'Connor, Jack Bartram, Sujith Samarasinghe, Ajay Vora, and Nick Goulden, Great Ormond Street Hospital; Rachael Hough, University College Hospital, London; Amir Enshaei, Christine J. Harrison, Claire Schwab, and Anthony V. Moorman, Northern Institute for Cancer Research, Newcastle University, Newcastle upon Tyne; Jeremy Hancock, North Bristol National Health Service Trust; John Moppett, Royal Hospital for Sick Children, Bristol; Ajay Vora, Sheffield Children's Hospital, Sheffield; Rachel Wade, Medical Research Council, University of Oxford, Oxford, United Kingdom; and Nick Goulden, Trapehade, Monferran-Plavès, France.
J Clin Oncol. 2018 Jan 1;36(1):34-43. doi: 10.1200/JCO.2017.74.0449. Epub 2017 Nov 13.
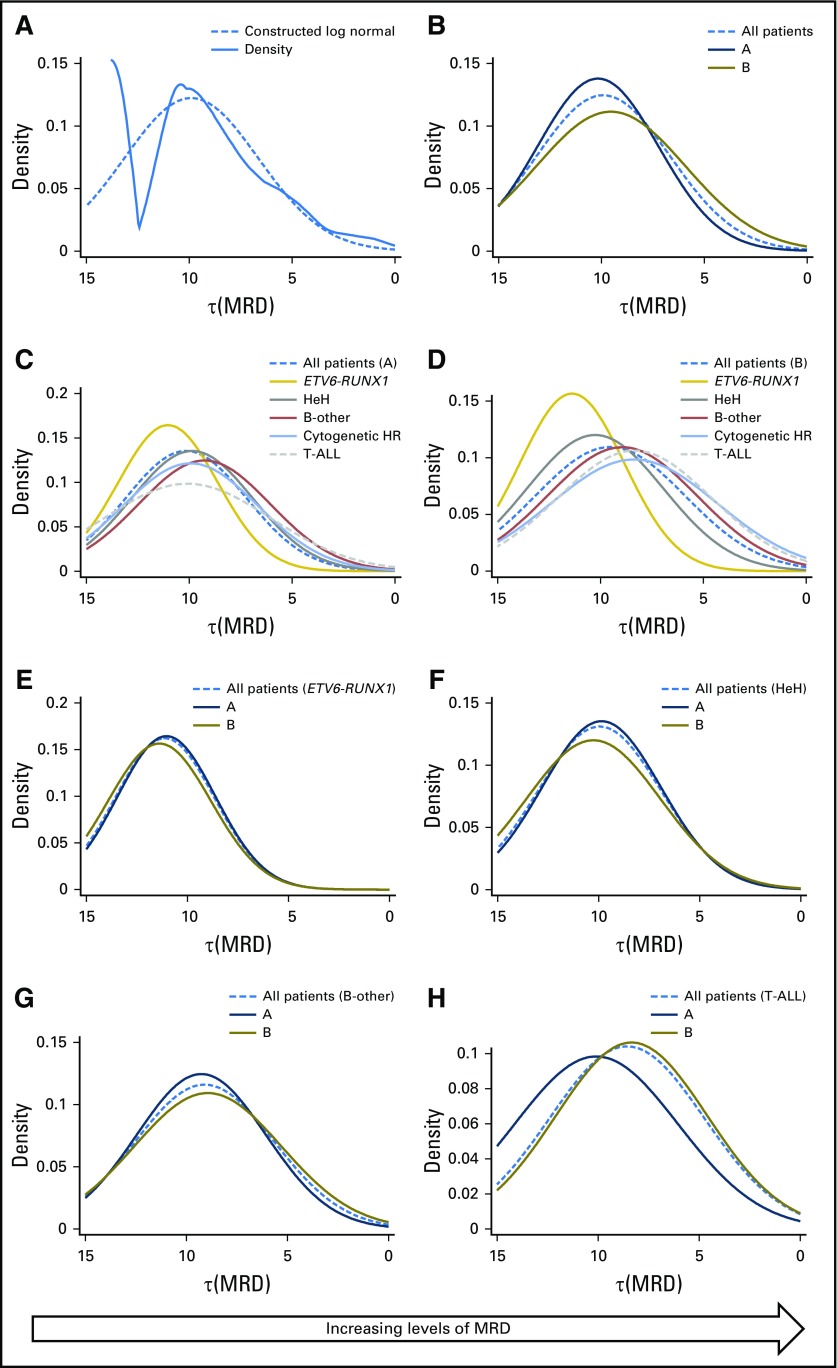
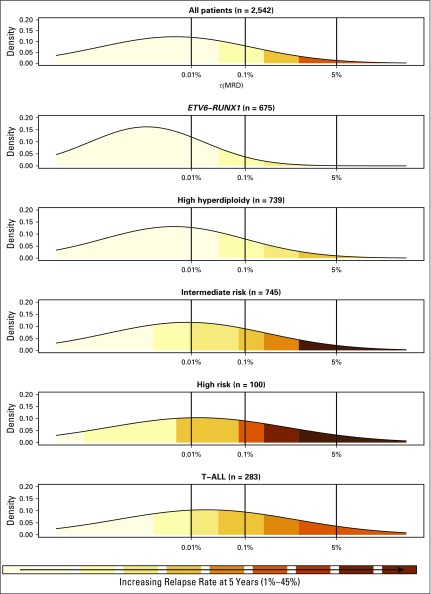
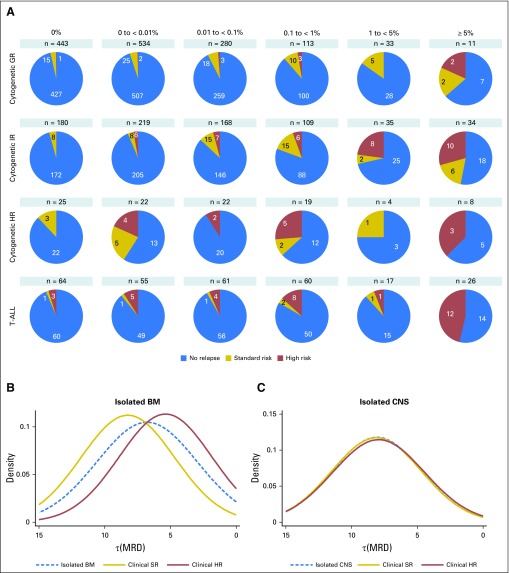
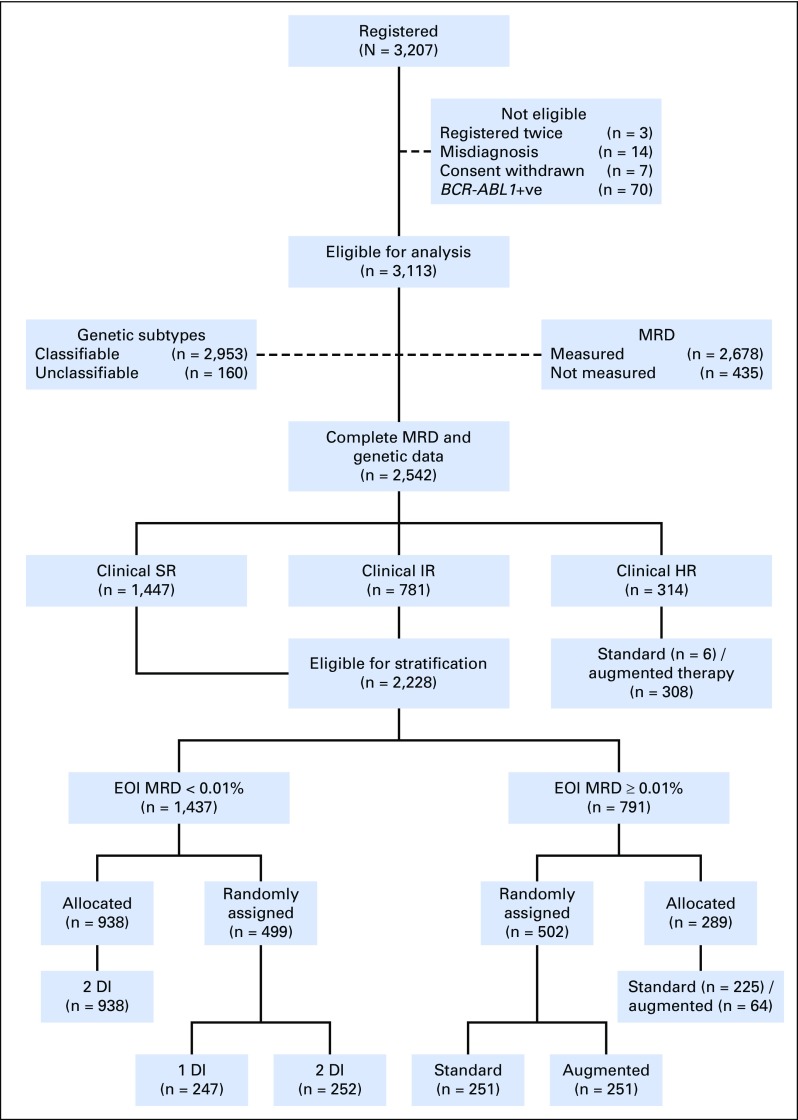
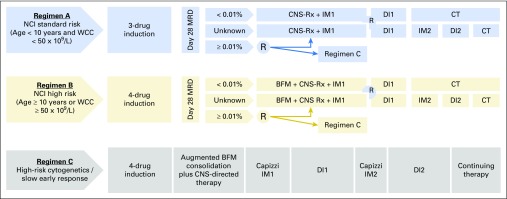
Purpose Minimal residual disease (MRD) and genetic abnormalities are important risk factors for outcome in acute lymphoblastic leukemia. Current risk algorithms dichotomize MRD data and do not assimilate genetics when assigning MRD risk, which reduces predictive accuracy. The aim of our study was to exploit the full power of MRD by examining it as a continuous variable and to integrate it with genetics. Patients and Methods We used a population-based cohort of 3,113 patients who were treated in UKALL2003, with a median follow-up of 7 years. MRD was evaluated by polymerase chain reaction analysis of Ig/TCR gene rearrangements, and patients were assigned to a genetic subtype on the basis of immunophenotype, cytogenetics, and fluorescence in situ hybridization. To examine response kinetics at the end of induction, we log-transformed the absolute MRD value and examined its distribution across subgroups. Results MRD was log normally distributed at the end of induction. MRD distributions of patients with distinct genetic subtypes were different ( P < .001). Patients with good-risk cytogenetics demonstrated the fastest disease clearance, whereas patients with high-risk genetics and T-cell acute lymphoblastic leukemia responded more slowly. The risk of relapse was correlated with MRD kinetics, and each log reduction in disease level reduced the risk by 20% (hazard ratio, 0.80; 95% CI, 0.77 to 0.83; P < .001). Although the risk of relapse was directly proportional to the MRD level within each genetic risk group, absolute relapse rate that was associated with a specific MRD value or category varied significantly by genetic subtype. Integration of genetic subtype-specific MRD values allowed more refined risk group stratification. Conclusion A single threshold for assigning patients to an MRD risk group does not reflect the response kinetics of the different genetic subtypes. Future risk algorithms should integrate genetics with MRD to accurately identify patients with the lowest and highest risk of relapse.
目的 微小残留病(MRD)和遗传异常是急性淋巴细胞白血病(ALL)预后的重要危险因素。目前的风险算法将 MRD 数据二分法,并在分配 MRD 风险时不整合遗传学,从而降低了预测准确性。我们的研究旨在通过将 MRD 作为连续变量进行检查,并将其与遗传学相结合,充分利用 MRD 的力量。
患者和方法 我们使用了英国 ALL2003 中的 3113 名患者的基于人群的队列,中位随访时间为 7 年。通过聚合酶链反应分析 Ig/TCR 基因重排评估 MRD,根据免疫表型、细胞遗传学和荧光原位杂交将患者分配到遗传亚型。为了检查诱导结束时的反应动力学,我们对绝对 MRD 值进行了对数转换,并检查了其在亚组中的分布。
结果 在诱导结束时,MRD 呈对数正态分布。具有不同遗传亚型的患者的 MRD 分布不同(P <.001)。具有良好风险细胞遗传学的患者疾病清除最快,而具有高风险遗传学和 T 细胞急性淋巴细胞白血病的患者反应较慢。复发风险与 MRD 动力学相关,疾病水平每降低一个对数,风险降低 20%(风险比,0.80;95%置信区间,0.77 至 0.83;P <.001)。尽管每个遗传风险组中复发风险与 MRD 水平成正比,但与特定 MRD 值或类别相关的绝对复发率因遗传亚型而异。整合遗传亚型特异性 MRD 值可实现更精细的风险组分层。
结论 将患者分配到 MRD 风险组的单一阈值并不能反映不同遗传亚型的反应动力学。未来的风险算法应将遗传学与 MRD 相结合,以准确识别复发风险最低和最高的患者。