Kwon Hyungjoo, Choi Kyu-Sun, Yi Hyeong-Joong, Chun Hyoung-Joon, Lee Young-Jun, Kim Dong-Won
Department of Neurosurgery, Hanyang University College of Medicine, Seoul, Korea.
Department of Radiology, Hanyang University College of Medicine, Seoul, Korea.
J Korean Neurosurg Soc. 2017 Nov;60(6):723-729. doi: 10.3340/jkns.2017.0506.011. Epub 2017 Oct 25.
Acute subdural hematoma (ASDH) is generally considered a condition that should be managed surgically. However, some patients initially receive conservative treatment, a subset of whom require surgical intervention later. This study aimed to evaluate the predictors of delayed surgical intervention in ASDH patients who are initially managed conservatively.
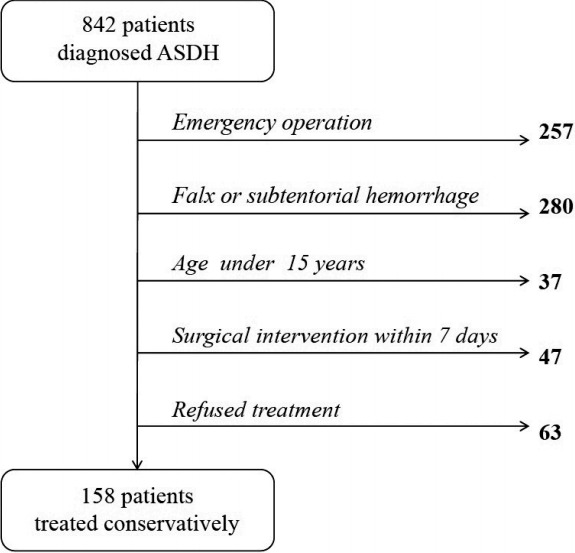
From January 2007 to December 2015, 842 patients diagnosed with ASDH were treated at our institution. Among them, 158 patients with convexity ASDH were initially treated conservatively. Patients were divided into a delayed surgery group and a conservative group. Demographic characteristics, past medication and medical histories, and radiological and laboratory data were collected by retrospective chart review. Independent risk factors were identified with univariate and multivariate analyses.
Twenty-eight patients (17.7%) underwent delayed surgical intervention. Their mean age was 69.0 years, and 82.1% were male. Hypertension, diabetes mellitus, and heart disease prevalence and use of anti-platelet agents did not significantly differ from the conservative group. However, age (=0.024), previous cerebral infarction history (=0.026), increased maximal hematoma thickness (<0.001), midline shifting (=0.001) and accompanying subarachnoid hemorrhage (=0.022) on initial brain computed tomography (CT) scan, low hemoglobin level (<0.001), high leukocyte count (=0.004), and low glucose level (=0.002) were significantly associated with delayed surgical intervention. In multivariate analysis, increased maximal hematoma thickness (odds ratio [OR]=1.279, 95% confidence interval [CI] 1.075-1.521; =0.006), low hemoglobin level (OR=0.673, 95% CI 0.467-0.970; =0.034), and high leukocyte count (OR=1.142, 95% CI 1.024-1.272; =0.017) were independent risk factors for delayed surgical intervention.
Due to the high likelihood of delayed surgical intervention among minimal ASDH patients with a thicker hematoma on initial brain CT, lower hemoglobin level, and higher leukocyte count, these patients should receive more careful observation.
急性硬膜下血肿(ASDH)一般被认为是一种需要手术治疗的疾病。然而,一些患者最初接受保守治疗,其中一部分患者后来需要手术干预。本研究旨在评估最初接受保守治疗的ASDH患者延迟手术干预的预测因素。
2007年1月至2015年12月,我院共治疗842例诊断为ASDH的患者。其中,158例凸面ASDH患者最初接受保守治疗。将患者分为延迟手术组和保守治疗组。通过回顾性病历审查收集人口统计学特征、既往用药和病史以及影像学和实验室数据。通过单因素和多因素分析确定独立危险因素。
28例患者(17.7%)接受了延迟手术干预。他们的平均年龄为69.0岁,82.1%为男性。高血压、糖尿病、心脏病患病率和抗血小板药物的使用与保守治疗组无显著差异。然而,年龄(=0.024)、既往脑梗死病史(=0.026)、初始脑计算机断层扫描(CT)上血肿最大厚度增加(<0.001)、中线移位(=0.001)以及伴有蛛网膜下腔出血(=0.022)、血红蛋白水平低(<0.001)、白细胞计数高(=0.004)和血糖水平低(=0.002)与延迟手术干预显著相关。多因素分析显示,血肿最大厚度增加(比值比[OR]=1.279,95%置信区间[CI]1.075 - 1.521;=0.006)、血红蛋白水平低(OR=0.673,95%CI 0.467 - 0.970;=0.034)和白细胞计数高(OR=1.142,95%CI 1.024 - 1.272;=0.017)是延迟手术干预的独立危险因素。
由于初始脑CT显示血肿较厚、血红蛋白水平较低且白细胞计数较高的轻度ASDH患者延迟手术干预的可能性较大,这些患者应接受更密切的观察。