Department of Neurosurgery, University Neurosurgical Center Holland (UNCH), Leiden University Medical Center & Haaglanden Medical Center & Haga Teaching Hospital, Leiden/The Hague, The Netherlands.
Department of Public Health, Erasmus Medical Center, Rotterdam, The Netherlands.
Acta Neurochir (Wien). 2019 May;161(5):875-884. doi: 10.1007/s00701-019-03878-5. Epub 2019 Mar 28.
The decision whether to operate or not in patients with a traumatic acute subdural hematoma (t-ASDH) can, in many cases, be a neurosurgical dilemma. There is a general conception that operating on severe cases leads to the survival of severely disabled patients and is associated with relatively high medical costs. There is however little information on the quality of life of patients after operation for t-ASDH, let alone on the cost-effectiveness.
This study retrospectively investigated patient outcome and in-hospital costs for 108 consecutive patients with a t-ASDH. Patient outcome was assessed using the Glasgow Outcome Score (GOS) and the Traumatic Brain Injury (TBI)-specific QOLIBRI questionnaire. The in-hospital costs were calculated using the Dutch guidelines for costs calculation.
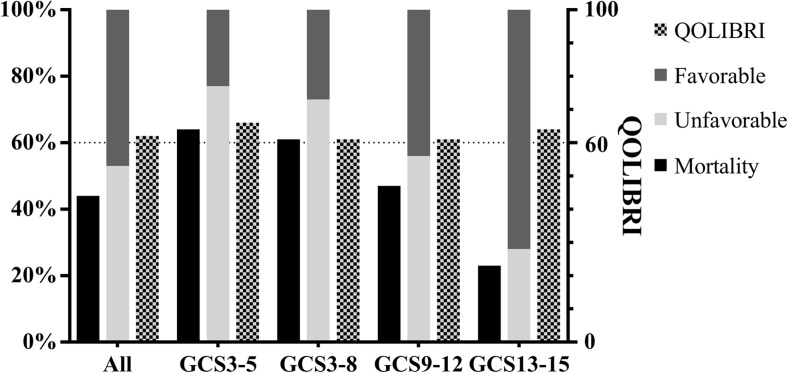
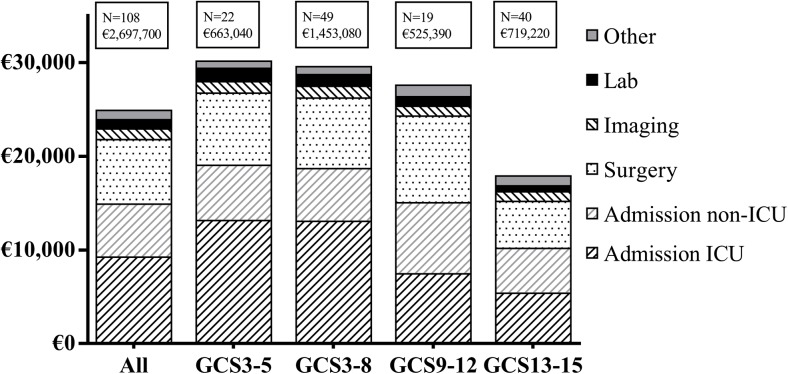
Out of 108 patients, 40 were classified as having sustained a mild (Glasgow Coma Scale (GCS) 13-15), 19 a moderate (GCS 9-12), and 49 a severe (GCS 3-8) TBI. As expected, mortality rates increased with higher TBI severity (23%, 47%, and 61% respectively), whereas the chance for favorable outcome (GOS 4-5) decreased (72%, 47%, and 29%). Interestingly, the mean QOLIBRI scores for survivors were quite similar between the TBI severity groups (61, 61, and 64). Healthcare consumption and in-hospital costs increased with TBI severity. In-hospital costs were relatively high (€24,980), especially after emergency surgery (€28,670) and when additional ICP monitoring was used (€36,580).
Although this study confirms that outcome is often "unfavorable" after t-ASDH, it also shows that "favorable" outcome can be achieved, even in the most severely injured patients. In-hospital treatment costs were substantial and mainly related to TBI severity, with admission and surgery as main cost drivers. These results serve as a basis for necessary future research focusing on the value-based cost-effectiveness of surgical treatment of patients with a t-ASDH.
在创伤性急性硬脑膜下血肿(t-ASDH)患者中,是否进行手术治疗在很多情况下都是神经外科的难题。人们普遍认为,对严重病例进行手术治疗会导致严重残疾患者存活,但也会带来相对较高的医疗费用。然而,关于 t-ASDH 手术后患者的生活质量信息甚少,更不用说成本效益了。
本研究回顾性调查了 108 例连续 t-ASDH 患者的患者结局和住院费用。使用格拉斯哥结局量表(GOS)和创伤性脑损伤(TBI)特异性 QOLIBRI 问卷评估患者结局。住院费用使用荷兰成本计算指南进行计算。
在 108 例患者中,40 例患者被归类为轻度(格拉斯哥昏迷量表(GCS)13-15),19 例为中度(GCS 9-12),49 例为重度(GCS 3-8)TBI。不出所料,死亡率随着 TBI 严重程度的增加而增加(分别为 23%、47%和 61%),而良好结局(GOS 4-5)的机会则降低(分别为 72%、47%和 29%)。有趣的是,幸存者的 QOLIBRI 平均得分在 TBI 严重程度组之间相当相似(61、61 和 64)。医疗保健消耗和住院费用随着 TBI 严重程度的增加而增加。住院费用相对较高(€24980),尤其是在急诊手术后(€28670)和使用颅内压监测时(€36580)。
尽管本研究证实 t-ASDH 后结局通常“不理想”,但也表明即使是最严重受伤的患者也可以实现“理想”结局。住院治疗费用很高,主要与 TBI 严重程度相关,入院和手术是主要的成本驱动因素。这些结果为未来关注手术治疗 t-ASDH 患者的基于价值的成本效益比的必要研究提供了依据。