Unit of Melanoma, Cancer Immunotherapy and Innovative Therapy, IRCCS Istituto Nazionale Tumori "Fondazione G. Pascale", Naples, Italy.
Istituto Nazionale Tumori di Napoli Fondazione "G. Pascale", Via Mariano Semmola, 80131, Naples, Italy.
J Transl Med. 2017 Nov 16;15(1):236. doi: 10.1186/s12967-017-1341-2.
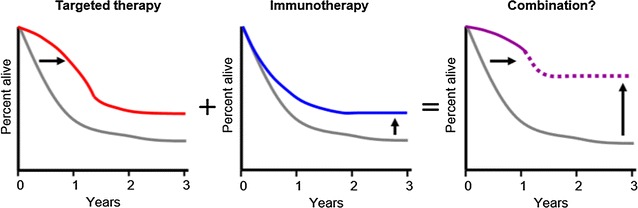
Major advances have been made in the treatment of cancer with targeted therapy and immunotherapy; several FDA-approved agents with associated improvement of 1-year survival rates became available for stage IV melanoma patients. Before 2010, the 1-year survival were quite low, at 30%; in 2011, the rise to nearly 50% in the setting of treatment with Ipilimumab, and rise to 70% with BRAF inhibitor monotherapy in 2013 was observed. Even more impressive are 1-year survival rates considering combination strategies with both targeted therapy and immunotherapy, now exceeding 80%. Can we improve response rates even further, and bring these therapies to more patients? In fact, despite these advances, responses are heterogeneous and are not always durable. There is a critical need to better understand who will benefit from therapy, as well as proper timing, sequence and combination of different therapeutic agents. How can we better understand responses to therapy and optimize treatment regimens? The key to better understanding therapy and to optimizing responses is with insights gained from responses to targeted therapy and immunotherapy through translational research in human samples. Combination therapies including chemotherapy, radiotherapy, targeted therapy, electrochemotherapy with immunotherapy agents such as Immune Checkpoint Blockers are under investigation but there is much room for improvement. Adoptive T cell therapy including tumor infiltrating lymphocytes and chimeric antigen receptor modified T cells therapy is also efficacious in metastatic melanoma and outcome enhancement seem likely by improved homing capacity of chemokine receptor transduced T cells. Tumor infiltrating lymphocytes therapy is also efficacious in metastatic melanoma and outcome enhancement seem likely by improved homing capacity of chemokine receptor transduced T cells. Understanding the mechanisms behind the development of acquired resistance and tests for biomarkers for treatment decisions are also under study and will offer new opportunities for more efficient combination therapies. Knowledge of immunologic features of the tumor microenvironment associated with response and resistance will improve the identification of patients who will derive the most benefit from monotherapy and might reveal additional immunologic determinants that could be targeted in combination with checkpoint blockade. The future of advanced melanoma needs to involve education and trials, biobanks with a focus on primary tumors, bioinformatics and empowerment of patients and clinicians.
在癌症的靶向治疗和免疫治疗方面已经取得了重大进展;几种获得 FDA 批准的药物,可显著提高 IV 期黑色素瘤患者的 1 年生存率。在 2010 年之前,这些患者的 1 年生存率相当低,为 30%;2011 年,在使用伊匹单抗治疗的情况下,这一数字上升到近 50%,而在 2013 年使用 BRAF 抑制剂单药治疗时,这一数字上升到 70%。更令人印象深刻的是,考虑到靶向治疗和免疫治疗的联合策略,1 年生存率现在超过了 80%。我们能否进一步提高缓解率,让更多的患者受益于这些疗法?事实上,尽管取得了这些进展,但这些反应是异质的,并不总是持久的。我们迫切需要更好地了解谁将从治疗中受益,以及适当的时机、不同治疗药物的顺序和组合。我们如何更好地了解治疗反应并优化治疗方案?通过对人类样本进行转化研究,从靶向治疗和免疫治疗的反应中获得的见解是更好地理解治疗和优化反应的关键。包括化疗、放疗、靶向治疗、电化学治疗与免疫治疗药物(如免疫检查点抑制剂)联合的联合治疗正在研究中,但仍有很大的改进空间。过继性 T 细胞治疗,包括肿瘤浸润淋巴细胞和嵌合抗原受体修饰 T 细胞治疗,在转移性黑色素瘤中也有效,通过转导趋化因子受体的 T 细胞归巢能力的提高,结果增强似乎是可能的。肿瘤浸润淋巴细胞治疗在转移性黑色素瘤中也有效,通过转导趋化因子受体的 T 细胞归巢能力的提高,结果增强似乎是可能的。了解获得性耐药的机制以及用于治疗决策的生物标志物检测也在研究中,这将为更有效的联合治疗提供新的机会。与反应和耐药相关的肿瘤微环境免疫特征的知识将提高识别从单药治疗中获益最多的患者的能力,并可能揭示可与检查点阻断联合靶向的其他免疫决定因素。晚期黑色素瘤的未来需要涉及教育和试验、关注原发性肿瘤的生物库、生物信息学以及增强患者和临床医生的能力。