Moreau Brigitte, Clement Pierre, Theoret Yves, Seidman Ernest G
Advanced IBD Fellow, Division of Gastroenterology, McGill University Health Center, Departments of Medicine and Pediatrics, Montreal, QC, Canada.
Division of Gastroenterology, Gatineau Hospital, Gatineau, QC, Canada.
Therap Adv Gastroenterol. 2017 Nov;10(11):819-827. doi: 10.1177/1756283X17733657. Epub 2017 Oct 11.
Thiopurines, azathioprine (AZA) and 6-mercaptopurine (6-MP) are common maintenance medications for inflammatory bowel disease (IBD). Excessive methylation thiopurine methyltransferase (TPMT) frequently causes therapeutic failure. Allopurinol reduces excessive 6-methyl-mercaptopurine (6-MMP) while enhancing 6-thioguanine (6-TGN) levels. The aim of this study was to evaluate clinical, metabolic and endoscopic impact of allopurinol in combination with low-dose thiopurine in IBD.
Retrospective review of consecutive cases treated with allopurinol. Metabolites and their ratios (6-MMP/6-TGN) were compared pre- and post-allopurinol. Clinical and endoscopic remission were assessed.
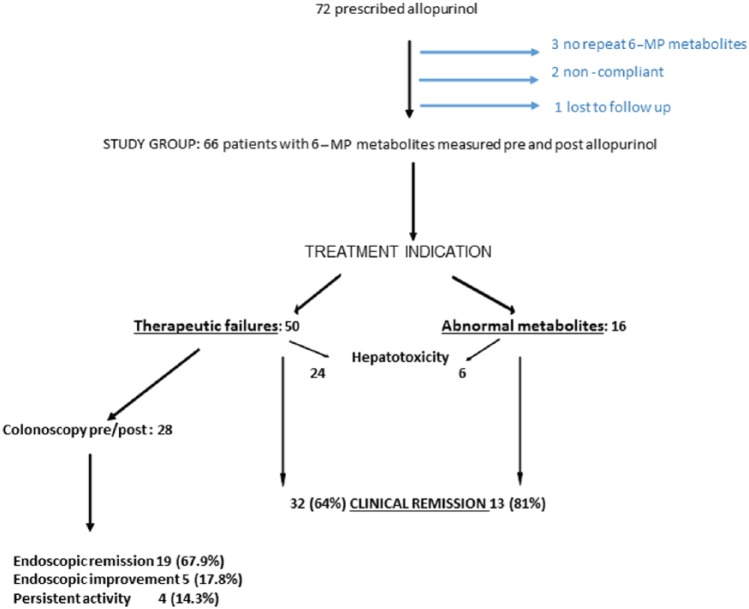
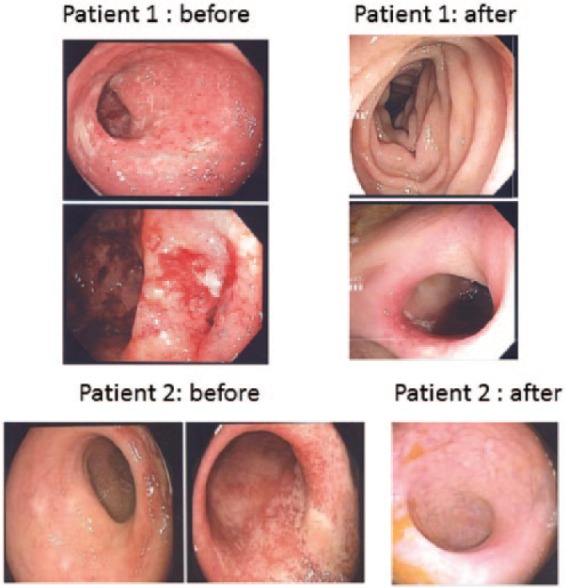
Allopurinol ( = 66) reduced mean dose of AZA by 70% ( < 0.01). Baseline levels (SD) 6-TGN, 6-MMP and 6-MMP/6-TGN were 165 (64), 9388 (5234) and 59.8 (30.3), respectively. These values improved on allopurinol to 297 (102), 896 (1031) and 3.4 (4.0), respectively ( < 0.0001). Therapeutic 6-TGN level (>235) was achieved in 49/58 cases on allopurinol combination therapy, 9/58 monotherapy ( = 0.0001). Among the thiopurine failure group (40 patients), clinical remission or response was observed in 65% and 22% of patients, respectively. In the asymptomatic group with excessive 6-MMP, 11/14 achieved sustained remission on allopurinol. Repeat colonoscopy ( = 28) showed mostly endoscopic remission (67.9%) or improvement (17.8%). Few had unimproved lesions (14.3%). Importantly, 46% of cases had complete mucosal healing. Two patients had cancer on combination therapy (de novo pancreatic cancer and fatal recurrence of metastatic testicular cancer). Elevated transaminases were reduced on allopurinol (48.2 6.9%) ( < 0.001); no change in leukopenic or infectious events occurred.
Allopurinol in combination with low-dose thiopurine corrected excessive 6-MMP levels, resulting in clinical remission and mucosal healing in the majority of cases. The potential cancer risk of allopurinol and thiopurine combination therapy needs further research.
硫唑嘌呤(AZA)和6-巯基嘌呤(6-MP)是炎症性肠病(IBD)常用的维持治疗药物。硫嘌呤甲基转移酶(TPMT)过度甲基化常导致治疗失败。别嘌醇可降低过量的6-甲基巯基嘌呤(6-MMP)水平,同时提高6-硫鸟嘌呤(6-TGN)水平。本研究旨在评估别嘌醇联合低剂量硫嘌呤对IBD患者的临床、代谢及内镜影响。
回顾性分析连续接受别嘌醇治疗的病例。比较别嘌醇治疗前后代谢产物及其比值(6-MMP/6-TGN)。评估临床及内镜缓解情况。
别嘌醇(n = 66)使AZA平均剂量降低70%(P < 0.01)。基线时6-TGN、6-MMP及6-MMP/6-TGN水平(标准差)分别为165(64)、9388(5234)及59.8(30.3)。使用别嘌醇后这些值分别改善为297(102)、896(1031)及3.4(4.0)(P < 0.0001)。别嘌醇联合治疗的58例患者中有49例达到治疗性6-TGN水平(>235),单药治疗的58例中有9例(P = 0.0001)。在硫嘌呤治疗失败组(40例患者)中,分别有65%和22%的患者出现临床缓解或反应。在6-MMP过量的无症状组中,14例患者中有11例使用别嘌醇后实现持续缓解。重复结肠镜检查(n = 28)显示大多为内镜缓解(67.9%)或改善(17.8%)。少数病变无改善(14.3%)。重要的是,46%的病例实现了完全黏膜愈合。联合治疗中有2例患者发生癌症(新发胰腺癌和转移性睾丸癌致命复发)。别嘌醇治疗后转氨酶升高情况有所改善(48.2±6.9%)(P < 0.001);白细胞减少或感染事件无变化。
别嘌醇联合低剂量硫嘌呤可纠正过量的6-MMP水平,多数情况下可实现临床缓解及黏膜愈合。别嘌醇与硫嘌呤联合治疗潜在的癌症风险需进一步研究。